Download
1 / 18
190 likes | 228 Views
Explore evidence-based practice, clinical decision-making, and evaluation of splinting for PIP joint flexion contractures. Case studies and Southlake Regional Health Centre hand program highlighted for in-depth understanding.

E N D
PRINCIPLES OF SPLINTING PIP JOINT FLEXION CONTRACTURES Virginia Tottenham BScPT CHT Lucy Winston BScOT Reg (Ont) CHT
OVERVIEW • INTRODUCTION • EVIDENCE BASED PRACTICE • CLINICAL DECISION MAKING • EVALUATION • CASE PRESENTATIONS • CONCLUSIONS
EVIDENCED BASED PRACTICE • What is it? • Lack of scientific studies • Biology of scar • Torque angle curve measurements • T.E.R.T.
CLINICAL DECISION MAKING • Efficacy • Compliance • Cost Effectiveness
EFFICACY • Stage of healing • Clinical experience • Evaluation
COMPLIANCE • Patient convenience • Comfort • Splint cosmesis
COST EFFECTIVENESS • Material costs • Therapist’s time • Patient’s time
EVALUATION • Expected outcome • Clinical change • Patient satisfaction
SOUTHLAKE REGIONAL HEALTH CENTRE HAND PROGRAM • Hand therapy model of care • Early intervention • Close communication with referring specialists and family physicians • Home program emphasized ++; modalities as needed • English speaking patients, within 45 min of hospital
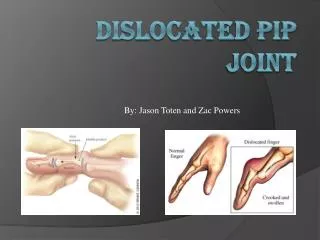
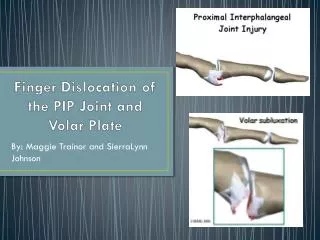
CASE STUDY #1 • 17 yr old RHD female student & competitive hockey player • Hyper-extension injury to (R) D5 PIP • Presented to hand therapy 3 months post-injury with flexion contracture D5 • Springy end feels, edema and pain after sports
Rx at initial ax: Night serial static extension digit splint CASE STUDY #1
AROM PIP initial: D5 30/70 AROM PIP @ d/c: D5 10/100 CASE STUDY #1
CASE STUDY #2 • 36 year old RHD mill worker • Jan 2002 sustained a saw injury (R) hand: • PIP joint injury D3 (bone loss) • PIP collateral ligament injury D3 • Flexor/extensor tendon injury D3 • Intrinsic muscle injury D3 • Common digital nerve injuries
CASE STUDY #2 • May 2002: Hunter’s Rod insertion D3 • September 2002: Tendon graft to D3 • December 2002: increased D3 PIP flexion contracture noted despite use of volar, hand based extension splint @ night (since injury)
Rx: Orfit extension splint (serial static circumferential) 23 hours per day CASE STUDY #2
Decreased compliance with orfit splint Rx: Capener splint (pre-fab dynamic) in day Orfit splint at night CASE STUDY #2
CASE STUDY #2 • Patient stopped wearing splint • Contracture increased • Increased wear of capener splint in day • Orfit splint at night
CONCLUSION • Base splint choice on literature , scar biology, assessment of the joint • Individualize treatment • Severity of injury • Surgery?