Download
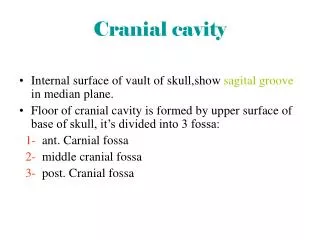
1 / 58
580 likes | 845 Views
Cranial Trauma. Gabriel C. Tender, MD Assistant Professor of Clinical Neurosurgery Louisiana State University in New Orleans. Patient #1. Walked in the ER after being hit in the head Initial GCS 14 – E4 V4 M6 (confused, but could maintain conversation) Started vomiting in the ER

E N D
Cranial Trauma Gabriel C. Tender, MD Assistant Professor of Clinical Neurosurgery Louisiana State University in New Orleans
Patient #1 • Walked in the ER after being hit in the head • Initial GCS 14 – E4 V4 M6 (confused, but could maintain conversation) • Started vomiting in the ER • In CT scan he lost consciousness and GCS dropped to 9 – E2 V2 M5 (opening eyes to pain only, muttering sounds, localizing pain)
Patient #2 • Involved in football accident • GCS 10 – E2 V3 M5 • Localize pain on R, not moving L side as much
Patient #3 • Involved in high-speed MVA • Sedated and intubated in the field • Initial GCS 7 before sedation – E1 V1 M5
Cranial Trauma • What is the most important factor on physical examination? • Level of consciousness
Cranial Trauma • GCS stratification (max: E4 V5 M6) • 14-15 mild • 9-12 moderate • 3-8 severe • NB: A confused patient cannot have a GCS of 15 (verbal is 4, so his GCS is 14 at the most)
Moderate and Severe Head Injury • What else is important (in comatose patients)? • Lateralization • Blown pupil • Different reaction to pain (left vs. right) • Babinski on one side only • Rectal tone if a spinal cord injury is suspected
Exploratory Burrholes • Indication (rare) • Patient dying of rapid transtentorial herniation (ipsilateral blown pupil and/or contralateral paralysis or decerebration) not improved with mannitol and hyperventilation
Insertion Point • 13 cm from the nasion, or just behind the hair line • 3 cm from the midline (usually on the right), or midpupillary line • For ventriculostomies • Aim for the ipsilateral epicanthus to hit the frontal horn, or go perpendicular to the bone (“straight down”) to hit the body of the lateral ventricle • If you haven’t hit the ventricle by 5 cm, STOP! (you’re going in the wrong direction; pull out and choose a new direction)
ICP monitors – Integra (Licox) • Monitors both ICP and PaO2 • Is more difficult to insert and maintain • Has more drift
ICP monitors – Integra (Licox) • Tricks for insertion • Use the drill that comes in the ICP monitor box, NOT the one in the cranial access kit • When you drill, put the drill stop at about 1.3-1.5 cm (you have to go through the bone) • Make sure you puncture the dura • Don’t tighten the second knob until you’re done inserting the monitors • Take all the three stylets out before inserting the Camino fiberoptic ICP monitor • You will feel some resistance when you go through the dura; gently overcome it • Do not insert the monitor past the black dot • Once all three monitors are inserted, tighten the second knob
ICP monitors – Codman • Monitors ICP only • Is easy to insert and maintain • Has less drift
ICP monitors – Codman • Tricks for insertion • When you drill, put the drill stop at about 1.3-1.5 cm (you have to go through the bone) • Make sure you puncture the dura • Zero with the monitor tip in sterile water • Do not insert the monitor past 5 cm (put a black mark at 5 cm from the tip)