Download

1 / 20
200 likes | 314 Views
COMPARISON BETWEEN UK AND CR SERVICES FOR EARLY ABORTION. By Dr. T. Masaříková. Common features. Legality of abortion Woman ' s choice, consent necessary Two practitioners ' approval needed Availability in both public and private sector Accessibility, affordability

E N D
COMPARISON BETWEEN UK AND CR SERVICES FOR EARLY ABORTION By Dr. T. Masaříková
Common features • Legality of abortion • Woman's choice, consent necessary • Two practitioners' approval needed • Availability in both public and private sector • Accessibility, affordability • Methods (surgical termination) • General anaesthetic • Diagnosis (gestation) based on U/S
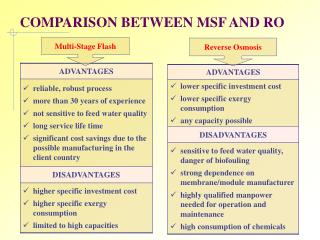
UK Both medical and surgical TOP Limit 24 weeks Free (NHS funded) Methods Dilation + electric suction aspiration (public sector) No dilation + manual suction aspiration (private sector) Choice of local anaesthetic and conscious sedation (private sector) Anti-D administration always Different methods depending on whether it is performed within NHS or private clinics CR No medical TOP Limit 12 weeks Service fee Methods Dilation + electric suction aspiration only General anaesthetic only Anti-D administration if more than 8 weeks Standardized methods – same procedures in both private and public sector Main differences
CR – General information • TOP can be requested by a woman who gives her consent in case of • Unwanted pregnancy • Foetal damage • Legal limit – 12 weeks (11+6) • „Mini TOP“ – up to 8 weeks (outpatient surgery, no anti-D administration, dilation + electric suction aspiration • TOP – Hospitalization (overnight, anti-D administration, electric suction aspiration) • „Mini TOP“ comprises 80% of all TOPs • Performed both in hospitals and private outpatient clinics • Service fee around 130 USD • Generally available, affordable, acceptable
CR in numbers (2006) • Total abortion rate – 25.352 cases • Population of CR – 10.287.189 • Birth rate – 105.800 • Abortion rate per 100 births – 24.0 • Age standardized abortion rate (per 1.000 resident women aged 15 – 44) – 18.3
CR - Tendencies • Abortion rate has a decreasing tendency 1970 – 1974 63 698 1990 – 1994 87 392 1975 – 1979 60 385 1995 – 1999 44 996 1980 – 1984 73 921 2000 – 2004 31 033 1985 – 1989 100 329 2005 26 443 2006 – 25 352
CR - Tendencies • Situation affected by fall of communist regime (availability of modern contraceptive methods) and general change of climate
70´s and 80´s Lack of modern contraceptive methods „Antibaby“ climate since 80´s Approval committees Highest abortion rate among women having 2 or 3 children 90´s – up to today Availability of modern contraceptive methods „Antibaby“ climate Woman's choice Highest abortion rate among nulliparous women CR - Tendencies
UK – General information • Women seeking a termination for whatever reason must have grounds under the Abortion Act 1967. A pregnancy may only be terminated if two registered medical practitioners are of the opinion, formed in good faith that an abortion is justified within the terms of the Act, in the light of their clinical judgement of all the particular circumstances of the individual case
UK – General information • Abortion is legal up to 23+6 • Gestation age based on U/S • Both medical and surgical abortions available • TOPs can be carried out both in NHS and authorized private clinics – methods might be different
Medical abortion in the UK • Introduced in 1991 • Early medical abortion (gestation up to 63 days) • Medical abortion in the late first trimester (9-13 weeks) • Mid-trimester abortion
Early medical abortion • Most effective method of abortion at gestations of less than 7 weeks • Continues to be an appropriate method for women in the 7-9 week gestation band • Misoprostol is a cost-effective alternative of E1 analogue gemeprost
Licensed use NHS Mifepristone 600mg(or 200mg) orally, followed 36-48 hours later by gemeprost 1 mg vaginally** Observation after PG administration Check-up in 1-3 weeks (beta-HCG, U/S) Unlicensed use Private and NHS clinics Mifepristone 200mg orally followed 1-3 days later by misoprostol 800µg vaginally (orally). 400 µg repeated orally or vaginally after 4h, if no expulsion Immediate discharge after PG administration No routine check-up (patient is given a pregnancy test to be carried out 3 weeks later) Early medical abortion
Early surgical abortion • Carried out by means of suction aspiration (using electric or manual suction) • Protocols include safeguards such as magnification of aspirate and follow-up serum beta-hCG • Choice of local anaesthetic, conscious sedation or general anaesthetic • Anti-D administration • No analgesics routinely offered • No cervical preparation (although beneficial if woman under 18 or at gestation of more than 10 weeks)
England and Wales in numbers (2006) • Total abortion rate – 193.700 cases • Population – 53.728.800 • Birth rate – 669.531 • Abortion rate per 100 births – 28.9 • Age standardized abortion rate (per 1.000 resident women aged 15 – 44) – 17.8
England and Wales • Abortion rate is steadily increasing 1971 94.6 1999173.7 1976 101.9 2000 175.5 1981 128.6 2001 176.4 1986 147.6 2002 175.0 1991 167.4 2003 181.6 1996 167.9 2004 185.7 1997 170.1 2005 186.4 1998 177.9 2006 193.7
UK Tendencies • Total abortion rate is increasing • Most of abortions funded by NHS • Most of abortions under 10 weeks • Proportion of medical terminations is increasing
England and Wales • Abortion rate highest at 35 per 1,000 for women age 19 • 87% of abortions funded by NHS; of these, just over half (55%) took place in the independent sector under NHS contract • 89% of abortions were carried out at under 13 weeks gestation; 68% were under 10 weeks • Medical abortion accounted for 30% of the total compared with 24% in 2005
Conclusions x controversies CR • Lacking availability of medical termination of pregnancy !!!!!!!! Reason? (Rigidity of current system?) • Misoprostol not available • Overnight hospitalization (8-12 weeks) Is it necessary?
Conclusions x controversies UK • Late pregnancy abortion – change of legal limits? • Availability – waiting times + costs • Promotion – abortion + contraception (esp. regarding immigrants) • Abortion Act – two registered practitioners needed • Medical TOP – self-administration of PG?