Download
1 / 80
800 likes | 1.34k Views
HEREDITARY ANEMIAS. PROF. SAMIYA NAEEMULLAH Diplomate American Board of Pediatrics FAAP, FCPS Head of Pediatrics Department Islamic International Medical College . ANEMIA. Defined as HB level below normal range Varies with age and sex of the individual Neonate Hb < 14 g/dl

E N D
HEREDITARY ANEMIAS PROF. SAMIYA NAEEMULLAH Diplomate American Board of Pediatrics FAAP, FCPS Head of Pediatrics Department Islamic International Medical College
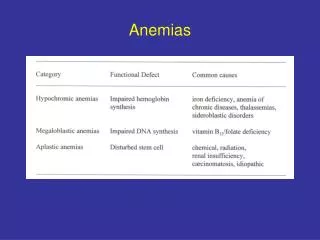
ANEMIA • Defined as HB level below normal range • Varies with age and sex of the individual • Neonate Hb < 14 g/dl • 1-12 months: Hb <10 g/dl • 1- 12 years Hb < 11 g/dl
IMPAIRED RED CELL PRODUCTION • Congenital Red cell aplasia • Diamond Blackfan Anemia • Fanconi Anemia
INCREASED RED CELL DESTRUCTION • Hemolytic Anemias • RED CELL MEMBRANE DISORDERS • Hereditary Spherocytosis • RED CELL ENZYME DISORDER • Glucose 6 – phosphate dehydrogenase deficiency (G6PD) • Hemoglobinopathies • Sickle cell disease • Thalassemia
LEARNING OBJECTIVES • Discuss the etiology of different types of hereditary anemias? • Differentiate between cell defects, enzymatic defects and hemoglobinopathies • Be able to distinguish the morphology of different hemolytic anemias • Discuss clinical features of sickle cell disease and Thalassemia Major • Correlate clinical features with pathophysiology of the disease
DIAMOND BLACKFAN ANEMIA • Etiology • Autosomal dominant 15% • Autosomal recessive 15% • Spradic 80% • FH 20%
CONGENITAL ANOMALIES Short stature
DIAGNOSIS • Low Hb% macrocyte • Low reticulocyte Count • Normal bilirubin • Absent red cell precussors on narrow
INHERITED APLASTIC ANEMIAS • Reduction or absence of all three main line in bone marrow leading to peripheral blood pancytopenia
FANCONI’S ANEMIA • Short stature • Abnormal radii & thumbs • Renal manifestation • Pigmented skin lesion • Increased chromosomal breakage of peripheral blood lymphocytes
Schwachman Diamond Syndrome • Autosomal Recessive disorder • Bone marrow failure • Pancreatic exocrine failure • Skeletal abnormalities
RED CELL MEMBRANE DISORDERS • Hereditary spherocytosis • Hereditary elliptocytosis
HEREDITARY SPHEROCYTOSIS • Autosomal dominant • No F/H – in 25% cases • Defect in genes for the skeletal proteins of the red cells membrane spectrin, ankyrin and band 3 red cell losses part of its membrane passing through spleen
in surface to volume ratio – causes the cells to become spheroidal. • Less deformable than normal RBS • Destruction in micro vasculature of the spleen
Jaundice at birth • Anemia • Mild to moderate splenomegaly • Aplastic crises • Gall stones
ENZYME DEFECTS • Glucose 6 phosphate dehydrogenase (G6PD) deficiency • Commonest red cell enzymopathy effecting over 100 million people world wide • G6PD in red cell essential for preventing • Oxidative damage to red cells • So cell lacking the enzyme are suseptible to oxidant induced hemolysis
Etiology with inherited as X linked effects males • G6PD activity in in Red cells • Mostly in old cells
CLINICALLY • Neonatal Jaundice • Acute hemolysis precipitected by • Drugs • Infection • Naphthalene in moth balls • Intravascular hemolysis • Fever, malaise, dark colored urine
HEMOGLOBINOPATHIES • These are red blood cell disorders which cause hemolytic anemia because of • Reduced or absent production of Hb A( & thalassemia) • Production of abnormal Hb e.g. sickle cell disease
BETA THALASSEMIA AUTOSOMAL RECESSIVE • Inherited disorder characterized by absence or decreased synthesis of beta globin chain of hemoglobin
Normal Fetal Hb at different ages • At birth – 70% • 5 weeks – 55% • 4 months – 10% • 5 month – 5% • At one year – (< 2%)
HETEROZYOUS SATE Thalassemia Minor • One normal betaglobin chain gene and one beta-thalassemia gene HOMOZYGOUS Thalassemia Intermedia • 2 Thalassemia genes Thalassemia Major • 2 Beta thalassemia genes
PATHOPHYSIOLOGY Beta Thalassemia minor • Most Common • Failure of one gene coding for beta chain • Alpha chain – production – normal • Alpha chain available combine with beta chain • Hb A levels
Excess alpha chain – stimulates production of delta chain – Hb A2 • Still excess alpha chains – switches off gamma chain production does not function correctly. And rate of gamma chain production is greater than in normal adult so amount of Hb F.
HbF • Poor oxygen deliverer and high affinity for O2 • Only functional Hb present is A2 Hypoxia Erythropoetin Stimulated marrow to maximum Extremedullary hematopaiesis Splenomegaly
CLINICAL MANIFESTATIONS Thalassemia Minor • The Growth & Development is normal • Mild anemia Hb – 10 mg./dl
Thalassemia Intermedia • Symptomatic by 2 – 4 yrs of age • Mod anemia • Thalassemic facies • Growth failure • Hepatosplenomegaly • Jaundice
THALASSEMIA MAJOR • DETROIT PEDIATRICIAN • 1925 THOMAS COOLEY (Cooley Anemia) • Profound anemia • Splenomegaly • Bony deformities • Greek word Thalasa SEA Blood
Universally fatal disease Is now converted into chronic illness
INCIDENCE • 3% of world’s population carry Thalassemia gene • PAKISTAN • Carrier rate 4-5% • Pathans 5.8% • Total No of patients 50,000-60,000 • 5000 – 6000 children are born each year
THALASSEMIA MAJOR • Born normal at birth • Starts getting pale,fussy,irritable • Starts refusing feeds
CLINICAL FEATURE • Bossing of skull • Maxillary overgrowth • Long face • Hepatosplenomegaly • Bones become thin • Fractures may occur • Heart failure
COMPLICATIONS • Iron Overload • Darkening of skin(Iron stimulated melanin) • Cardiomyopathy • Endocrinopathies • Infections (Hepatitis A,B,C,Malaria,HIV) • Failure to thrive • Antibody formation(10%)Alloantibodies