Download
1 / 17
170 likes | 545 Views
Helen Imseeh. N a i l p so r i a s i s. I n p so r i a s i s n a i l i n v o l v e m e n t i s c o mm on , m os t p a t i e n t s h a v e n a i l c h a n g e s a t so m e s t a g e

E N D
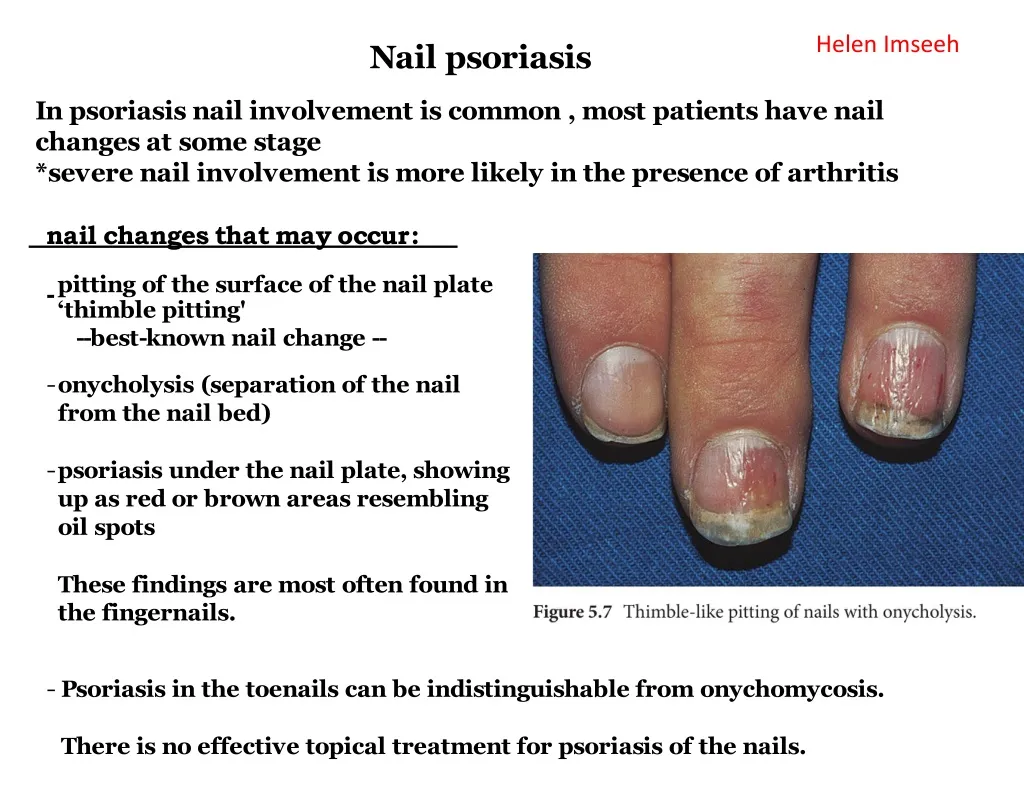
Helen Imseeh Nail psoriasis Inpsoriasisnail involvementiscommon,mostpatientshavenail changesatsomestage *severenail involvementismorelikelyin thepresenceofarthritis nailchangesthatmayoccur: -pittingofthesurfaceofthenail plate ‘thimblepitting' --best-knownnail change-- • onycholysis(separationofthenailfromthenail bed) • psoriasisunderthenail plate,showingupasredorbrownareasresemblingoil spots • Thesefindingsaremost oftenfoundinthefingernails. • Psoriasisinthetoenailscanbeindistinguishablefromonychomycosis. • Thereisnoeffectivetopical treatment forpsoriasisofthenails.
Bacterial infections staphylococcalinfections • Quickrevision • Staphylococciaregram-positivespherical cells • nonmotile • usuallyarrangedingrapelikeirregular clusters. • -Staphylococcusspeciesarefacultative Somearemembersof thenormal microbiotaof theskinandmucousmembranesofhumans suchas Staphylococcusaureuswhichfoundinaminoritywhocarryitintheirnostrils,perineumorarmpits.
Skindiseasescausedbystaphinfections Impetigo bothare highlycontagious Superficial bacterial skininfectionmaybecausedbyStaph.aureusorStreppyogenes It isthemost commonskininfectionofchildren occursparticularlyintropical orsubtropical regions,orduringsummermonthsinthenothernhemisphere. Primaryimpetigomainlyaffectsexposedareassuchas thefaceandhands,butmayalsoaffect trunk,perineumandotherbodysites
itisclassifiedasnonbullousorbullous largethin-walledbullacontainingserousyellowfluid. Itoftenrupturesleavingacompleteorpartiallydenudedareawitharingorarcofremainingbulla nonbulloustypepredominatesandpresentswithclusteroferosions, orsmallvesiclesorpustulesthathaveanadherentoroozing honey-yellowcrust. Asauseful ruleof thumb, thebulloustypeisusuallycausedby --Staphylococcusaureus thecrustedulcerated typeby--β-haemolyticstrainsofstreptococci.
aswesaidbefore thebullous typeisusuallycausedbyStaphylococcusaureus that'sbyproducingExfoliative toxinswhichcleavesuperficial skinadhesionmoleculedesmoglein1todisruptadhesionhighin the epidermis,causing thestratumcorneum tosloughoff. If the toxinislocalized thisproduces theblistersofbullousimpetigobut ifgeneralizedleads tomorewidespreadblisteringasin the staphylococcal scaldedskinsyndrome.
Course • Ittendstoclearevenwithouttreatment. • Complications • Streptococcalimpetigocantriggeranacuteglomerulonephritis. • Differentialdiagnosis • Herpessimplex • eczema. • Recurrentimpetigooftheheadandneck,forexample,shouldpromptasearchforscalplice. • Investigation • Thediagnosisisusuallymadeonclinicalgrounds. • Gramstainscanbedoneorswabscanbetakenforculture, • "buttreatmentmustnotbeheldupuntiltheresultsareavailable." • treatmentminorcases: • -removalofcrustsbycompressingthem • -applicationofatopicalantibioticsuchasneomycin,fusidicacid,mupirocinorbacitracin • severecases: • Systemicantibiotics(suchasflucloxacillin,erythromycinorcefalexin)orifanephritogenicstrainofstreptococcusissuspected(penicillinV).
Scaldedskinsyndrome Characterizedbyfeverandgeneralizederythematousrashand tendernesswhicharefollowedby thelooseningoflarge areasofoverlyingepidermis. ⊕ Nikolsky sign (gentle strokes result in exfoliation) Inchildren theconditionisusuallycausedbya toxinproducedbystaphylococcal infectionelsewhere(e.g.impetigoorconjunctivitis Seenin: -newbornsandchildren, -adultswithrenal insufficiency. mostadultshaveantibodiestothetoxin,andthereforeareprotected. Inadultswithwidespreadexfoliation,considertoxicepidermalnecrolysis, whichisusuallydrug-induced. Thedamagetotheepidermisintoxicepidermalnecrolysisisfullthickness, andaskinbiopsywilldistinguishitfromthescaldedskinsyndrome
Folliculitisisinflamedhairfollicles. Theresultisatenderredspot,oftenwithasurfacepustule.Folliculitis maybesuperficialordeep,andcanaffectanyhair-bearingareaofskin. Afuruncle(syn.boil)isadeeper,and morepronouncedinfectionofthehairfollicleinwhichpurulent materialextendsthroughthedermisintothesubcutaneoustissue,whereasmall abscessforms. Acarbuncleisacoalescenceofseveralinflamedfolliclesintoasingleinflammatory masswithpurulentdrainagefrom multiplefollicles
furuncle Adolescentboysareespeciallysusceptibletothem. Presentationandcourse Atenderrednoduleenlarges,andlater maydischargepusanditscentral‘core’ beforehealingtoleaveascar. Feverandenlargeddrainingnodesarerare. Mostpatientshaveoneortwoboilsonly,andthen clear.
Thesuddenappearanceofmanyfurunclessuggestsavirulentstaphlococcusincludingstrainsofcommunity-aquiredMRSA,orstaphylococciexpressing Panton–Valentineleucocidintoxin. Afewunfortunatepersonssufferfrom atiresomesequenceofboils(chronicfurunculosis),oftenduetosusceptibiltyoffolliclesorcolonizationofnaresorgroinswithpathogenicbacteria. Immunodeficiencyisrarelytheproblem. Complications Cavernoussinusthrombosisisanunusualcomplicationofboilsonthecentralface. Septicaemia mayoccurbutisrare. Investigations inchronicfurunculosis Generalexamination:lookforunderlyingskindisease(e.g.scabies,pediculosis,eczema). Testtheurineforsugar. Fullbloodcount. Cultureswabsfromlesionsandcarriersites(nostrils,perineum)ofthepatientandimmediatefamily. Testbothtoidentifytheorganism andtoevaluatesensitivitytovariousantibiotics. Immunologicalevaluationonlyifthepatienthasrecurrentorunusualinternalinfectionstoo.
Treatment Acuteepisodes: simpleincisionanddrainage. Anappropriatesystemicantibioticisneeded -when manyfurunclesareerupting -whenfeverispresent, -whenthepatientisimmunosuppressed. Inrecurrentfurunculosis: treatcarriersitessuchasthenosetwicedailyforthefirst5daysofeachmonthwithan appropriatetopicalantisepticorantibiotic(e.g.mupirocincream orfusidicacidointment)totrytoeliminatestaphylococcalcarriage. A10-daycourseofrifampicinmayalsohelperadicatecarriage. Treatfamilycarriersinthesameway. Instubbornchroniccaseslong-term treatmentwith sequentialtopicalandsystemicantibioticschosen tocoverorganism’sprovensensitivitieswillbeneeded. Dailybathusinganantisepticsoap. Improvehygieneandnutritionalstate,iffaulty.
Carbuncle • AgroupofadjacenthairfolliclesbecomesdeeplyinfectedwithStaphylococcusaureus,leadingtoaswollenpainfulsuppuratingareadischargingpusfromseveral points. • Thepainandsystemicupsetaregreaterthanthoseofaboil. • Diabetes mustbeexcluded. Treatment • needsbothtopicalandsystemicantibiotics. • Incisionanddrainagehasbeenshowntospeeduphealing, • Considerthepossibilityofafungalkerioninunresponsivecarbuncles.
Streptococcalinfections • Quickrevision • Staphylococciaregram-positivespherical cells • nonmotile • characteristicallyformpairsorchainsduringgrowth. • -somearemembersof thenormal humanmicrobiota
Erysipelas Infectioninvolvingupperdermisandsuperficial lymphatics,usuallyfromSpyogenes.Presentswithwell-defineddemarcationbetweeninfectedandnormal skin Thefirstwarningofanattackisoftenmalaise,shiveringandafever. Afterafewhourstheaffectedareaofskinbecomesred,andtheeruptionspreadswithawell-definedadvancingedge. Blistersmaydevelopontheredplaques
treatment Untreated, the condition can even be fatal, but itresponds rapidly to systemic penicillin, sometimes given intravenously. The choice of oral or parenteral route is dictatedby the severity of the infection. Recurrence occurs in up to 20% of erysipelas patients. Unlike lightning, erysipelas often strikes in the same place twice. Recurrent bouts may need long-term prophylactic penicillin
Cellulitis -Acute,painful,spreadinginfectionofdeeperdermisandsubcutaneoustissues. (deeperlevelthanerysipelas) -Usuallyfrom S pyogenesor S aureus. -Oftenstartswithabreakinskinfromtraumaoranotherinfection areaismoreraisedandswollen,and theerythemalessmarginated thaninerysipelas Toewebintertrigoandlymphoedemaareriskfactorsfor thedevelopmentofbotherysipelasandcellulitis,whichin turnpredisposepatients topersistentlymphoedema.Itisimportanttoget theseunderlyingfactorsaswell as thebacterial infection toreduce the risksofrecurrence.
Treatment: -elevationandrest -systemicantibiotics,sometimesgivenintravenouslyandactiveagainstbothstaphylococciandstreptococci. Acombinationofamacrolidewithastreptograminmaybemoreeffectivethanpenicillins.