Download
1 / 49
560 likes | 700 Views
BENIGN DISORDERS OF THE VULVA. Rukset Attar, MD, PhD Depar t ment of Obstetrics and Gynecology. Or i g i nates from ectoderm erithematous , ulcerative, proliferative and hyper k eratotic lesions Examined after application of 3-5% acetic acide or 1% toluidin blue

E N D
BENIGN DISORDERS OF THE VULVA Rukset Attar, MD, PhD Department of Obstetrics and Gynecology
Originates from ectoderm erithematous, ulcerative, proliferative and hyperkeratotic lesions Examined after application of 3-5% acetic acide or 1% toluidin blue Colposcopy is time consuming Biopsy from multiple sites with Keyes biopsy forceps
Benign Lesions of the Vulva • Inflamatory • Dermatities ( contact, seboreic-intertrigo, psoriasis, candidasis, tinea, infections of the major and minor vestibular glands) • Viral diseases ( HSV, HPV, Herpes Zoster, Molluscumcontagiosum) • Ulcerative lesions ( Crohn, Behcet, venerial diseases, nonspes lesions-hydradenitis, folliculitis,etc) • Traumatic • hematomas • lacerations
White • Depigmentation-vitiligo or leukoderma • Hypercheratotic lesions( inflamatory,benignneoplasms) • Vulvar dystrophies (Lichen sclerosus, squamous cell hyperplasia-hyperplasticdystrophy,mixt)
Benign Lesions of the Vulva • Benign neoplasms • Benign cystic tumors (Epidermal cysts, sebaceous cysts, apocrine sweat gland cysts, Skene duct cyst, urethral diverticulum, inguinal hernia, Gartner's duct cyst, Bartholin's duct cyst and abscess) • Benign solid tumors (Acrochordon, pigmented nevi, leiomyoma, fibroma, lipoma, neurofibromas, granular cell myoblastoma) • Vascular and lymphatic disease(Varicosities, hematoma, edema, granulomapyogenicum, hemangioma, lymphangioma)
Vulvar manifestation of systemic disease (Leukemia, dermatologic disorders (disseminated lupus erythematosus, pemphigusvulgaris) Infestations of the vulva (Pediculosis pubis, scabies, enterobiasis)
Vascular and lymphatic disease • varicosities • hematoma • edema • granuloma pyogenicum(a variant of a capillary hemangioma. It usually is single, raised, and dull red. Its size seldom exceeds 3 cm. Pyogenic granuloma is important because it tends to bleed easily if traumatized. Wide excisional biopsy is indicated to alleviate symptoms and to rule out a malignant melanoma) • hemangioma • lymphangioma
Vulvar manifestation of systemic disease • leukemia • dermatologic disorders (disseminated lupus erythematosus, pemphigus vulgaris, contact dermatitis, psoriasis) • obesity • Acanthosis nigricans is a benign hyperpigmented lesion characterized by papillomatous hypertrophy. It may be associated with an underlying adenocarcinoma. • Intertrigo is an inflammatory reaction involving the genitocrural folds or the skin under the abdominal panniculus. It is common in obese patients and results from persistent moistness of the skin surfaces.
Vulvar manifestation of systemic disease • Diabetes Mellitus • Diabetic vulvitis. It is caused by a chronic vulvovaginal candidiasis • Necrotizing fasciitis is seen most commonly in diabetics. It is an uncommon, acute, rapidly spreading, frequently fatal polymicrobial infection of the superficial fascia and subcutaneous fascia. It may be seen following a surgical procedure such as an episiotomy or after minor trauma. It presents as an extremely painful, tender, and indurated region with central necrosis and peripheral purplish erythema. Treatment requires surgical debridement and systemic antibiotics. • Behçet's syndrome
Viral Infections • Herpes genitalis • HPV • Herpes Zoster • MolluscumContagiosum
Herpes Zoster • A painful eruption of groups of vesicles is distributed over an area of skin corresponding to the course of 1 or more peripheral sensory nerves. • The causative agent is varicella-zoster virus. • The lesion is commonly unilateral and not infrequently attacks 1 buttock, 1 thigh, or 1 side of the vulva.
Molluscum Contagiosum • These benign epithelial poxvirus-induced tumors are dome-shaped, often umbilicated, and vary in size up to 1 cm. • The lesions often are multiple and are mildly contagious. • The microscopic appearance is characterized by numerous inclusion bodies (molluscum bodies) in the cytoplasm of the cells. • Each lesion can be treated by desiccation, freezing, or curettage and chemical cauterization of the base. • Topical imiquimod( aldara ) can be used as alternative therapy
Infestations of the Vulva • Pediculosis Pubis • The crab louse (Phthirus pubis) is transmitted through sexual contact or from shared infected bedding or clothing. • intense pubic and anogenital itching. • minute pale-brown insects and their ova may be seen attached to terminal hair shafts. • treatment consists of permethrin 1% cream, lindane 1% shampoo, or pyrethrins with piperonyl butoxide. • Lindane is not recommended for pregnant or lactating women or for children younger than 2 years. • Treat all contacts and sterilize clothing that has been in contact with the infested area.
Infestations of the Vulva • Scabies • Sarcoptes scabiei • itching and excoriation of the skin surfaces in the vicinity of minute skin burrows where parasites have deposited ova. • The itch mite is transmitted, often directly, from infected persons. • The patient should take a hot soapy bath, scrubbing the burrows and encrusted areas thoroughly. • Treatment consists of permethrin cream (5%), which should be applied to the entire body from the neck down, with particular attention to the hands, wrists, axillae, breasts, and anogenital region. It should be washed off after 8–14 hours.
Infestations of the Vulva • Alternatively, lindane (1%) in the lotion or cream form can be applied in a thin layer to all areas of the body and washed off after 8 hours. • All potentially infected clothing or bedding should be washed or dry-cleaned. • All contacts or persons in the family must be treated in the same way to prevent reinfection. • Therapy should be repeated in 10–14 days if new lesions develop.
Infestations of the Vulva • Enterobiasis (Pinworm, Seatworm) • Apply ammoniated mercury ointment to the perianal region twice daily for relief of itching. • Pinworms succumb to systemic treatment with pyrantel pamoate, mebendazole, or pyrvinium pamoate
Mycotic Infections of the Vulva • Fungal Dermatitis (Dermatophytoses) • Tinea cruris is a superficial fungal infection of the genitocrural area that is more common in men than in women. • The most common organisms are Trichophyton mentagrophytes and Trichophyton rubrum. • The initial lesions usually are located on the upper inner thighs and are well circumscribed, erythematous, dry, scaly areas that coalesce. • Scratching causes lichenification and a gross appearance similar to neurodermatitis.
Mycotic Infections of the Vulva • The diagnosis depends on microscopic examination (as for Candida) • Culture on Sabouraud's medium confirms the diagnosis. • Treatment with 1% haloprogin, tolnaftate, or a similar agent is effective. • Topical imidazole preparation at twice-daily application for 2–3 weeks also is highly effective
Other Infections of the Vulva • Impetigo • is caused by the hemolytic S aureus or streptococci. • The disease is autoinoculable and spreads quickly to other parts of the body, including the vulva. • Thin-walled vesicles and bullae develop that display reddened edges and crusted surfaces after rupture. • The disease is common in children, particularly on the face, hands, and vulva. • The patient must be isolated and the blebs incised or crusts removed aseptically. • Neomycin or bacitracin should be applied twice daily for 1 week. • Bathing with an antibacterial soap is recommended.
Other Infections of the Vulva • Furunculosis • Vulvar folliculitis is caused by a staphylococcal infection of hair follicles. • Furunculosis occurs if the infection spreads into the perifollicular tissues, producing a localized cellulitis. • Minor infections can be treated by applications of topical antibiotic lotions. • Deeper infections can be brought to a head with hot soaks, after which the pustules should be incised and drained. • Appropriate systemic antibiotics are warranted when extensive furunculosis is present.
Other Infections of the Vulva • Erysipelas • Erysipelas is a rapidly spreading erythematous lesion of the skin caused by invasion of the superficial lymphatics by β-hemolytic streptococci. • is extremely rare and is most commonly seen after trauma to the vulva or a surgical procedure. • Systemic symptoms of chills, fever, and malaise • Vesicles and bullae may appear, and erythematous streaks leading to the regional lymph nodes are typical. • The patient should be given systemic (preferably parenteral) penicillin or tetracycline orally in large doses
Other Infections of the Vulva • Hidradenitis • Hidradenitis suppurativa is a refractory process of the apocrine sweat glands, usually associated with staphylococci or streptococci. • Treatment early in the disease consists of drainage and administration of antibiotics based on organism sensitivity testing. • Long-term therapy with isotretinoin may be considered. • Antiandrogen therapy with cyproterone acetate or ethinyl estradiol may be an alternate but highly effective treatment.
Other Infections of the Vulva • Severe chronic infections may not respond to medical therapy, and the involved skin and subcutaneous tissues must be removed down to the deep fascia. • This may necessitate a filet and curettage or a complete vulvectomy. • The area generally will not heal after a primary closure; therefore, the wound must be left open and allowed to heal by secondary intention, or a split-thickness graft may be placed. • Squamous cell carcinoma is rarely associated with hidradenitis suppurativa.
Other Infections of the Vulva • Tuberculosis (Vulvovaginal Lupus Vulgaris) • is manifested by chronic, minimally painful, exudative "sores" that are tender, reddish, raised, moderately firm, and nodular, with central "apple jelly"-like contents • wet compresses of aluminum acetate solution (Burow's solution) are helpful. • systemic antituberculosis therapy should be given.
Vulvar Nonneoplastic Epithelial Disorders • Vulvar dystrophies was previously used to define the nonneoplastic epithelial disorders of the vulva. • As characterized by the International Society for the Study of Vulvovaginal Disease (ISSVD), these lesions include • lichen sclerosus (previously lichen sclerosus et atrophicus), • squamous cell hyperplasia (previously hyperplastic dystrophy), and • mixt
Vulvar Nonneoplastic Epithelial Disorders • These lesions present classically with intense pruritus with or without pain and vulvar epithelial changes. • Differentiating from among these disorders and ruling out an underlying malignant process require histopathologic diagnosis. • The risk of an underlying malignancy is less than 5%. • Patients must be reexamined periodically, and one should not hesitate to take additional biopsy specimens.
Vulvar Nonneoplastic Epithelial Disorders • Lichen sclerosus • Thin, white, wrinkled tissue, with a cigarette-paper appearance • Clobetasol propionate(dermovate) 0.05% twice daily for 3 months • 2% testosterone cream twice daily for 3 months • 1.25% topical progesterone twice daily for 3 months 9 esp for children-discontinue for 1 year at puberty and menapaosal women) • Intralesionaltriamcinolone injection5 mg in 2 ml or 10 mg in 1 ml injection 0.1 ml at diff sites with 22 gauge spinal needle • surgery
Vulvar Nonneoplastic Epithelial Disorders • Squamous cell hyperplasia • Circumscribed, single or multifocal • Raised white lesion on vulva or adjacent tissue (generally of labia majora and clitoris) • Medium-potency topical steroids twice daily ( kenocort-A, locacortene)- not eff then high-potency topical steroids(dermovate) twice daily when satisfactory relief established then hydrocortisone • With benadryl at bedtime and white cotton gloves • Intralesionaltriamcinolone injection5 mg in 2 ml or 10 mg in 1 ml injection 0.1 ml at diff sites with 22 gauge spinal needle • surgery
Vulvar Nonneoplastic Epithelial Disorders • Lichen simplex chronicus • Thickened white epithelium on vulva • Generally unilateral and localized • Medium-potency topical steroids twice a daily
Benign Cystic Tumors • Epidermal Cyst • epithelial cells-may result from traumatic suturing of skin fragments during closure of the vulvar mucosa and skin after trauma or episiotomy. • most epidermal cysts arise from occlusion of pilosebaceous ducts. • These cysts usually are small, solitary, and asymptomatic.
Benign Cystic Tumors • Sebaceous Cysts • develops when the sebaceous gland's duct becomes occluded and accumulation of the sebaceous material occurs. • are frequently multiple and almost always involve the labia majora. • are generally asymptomatic; however, acutely infected cysts may require incision and drainage.
Benign Cystic Tumors • Apocrine Sweat Gland Cysts • Occlusion of the ducts with keratin results in an extremely pruritic, microcystic disease called Fox-Fordyce disease. • Chronic infection in the apocrine glands, usually with staphylococci or streptococci, results in multiple painful subcutaneous abscesses and draining sinuses. This condition is called hidradenitis suppurativa, which is generally treated with a broad-spectrum antibiotic. • Hidradenoma and syringoma are included in a diverse group of benign cystic or solid tumors of apocrine sweat gland origin present as small subcutaneous and asymptomatic tumors.
Benign Cystic Tumors • Bartholin's Duct Cyst and Abscess • Obstruction of the main duct of Bartholin's gland results in retention of secretions and cystic dilatation. • Infection is an important cause of obstruction; however, other causes include inspissated mucus and congenital narrowing of the duct. • Secondary infection may result in recurrent abscess formation. • The gland and duct are located deep in the posterior third of each labium majus. Enlargement in the postmenopausal patient may represent a malignant process (although the incidence is < 1%), and biopsy should be considered
Benign Cystic Tumors • Other • Skene duct cyst • urethral diverticulum • An inguinal hernia • Occlusion of a persistent processus vaginalis (canal of Nuck) may cause a cystic tumor or hydrocele. • Dilatation of the mesonephric duct vestiges produces lateral vaginal wall cysts, Gartner's duct cyst. • Supernumerary mammary tissue that persists in the labia majora may form a cystic or solid tumor or even an adenocarcinoma; engorgement of such tissue in the pregnant patient can be symptomatic.
Benign Solid Tumors • Acrochordon • An acrochordon is a flesh-colored, soft polypoid tumor of the vulvar skin that has been called a fibroepithelial polyp or simply a skin tag. • The tumor does not become malignant and is of no clinical importance, unless it becomes traumatized, causing bleeding. • Simple excision biopsy in the office is ordinarily adequate therapy.
Benign Solid Tumors • Pigmented Nevus • Leiomyoma, Fibroma, and Lipoma • Neurofibroma - may be solitary, solid tumors of the vulva or associated with generalized neurofibromatosis (Recklinghausen's disease)-They arise from the neural sheath and usually are small lesions of no consequence
Benign Solid Tumors • Granular Cell Myoblastoma (Schwannoma)-is usually a solitary, painless, slow-growing, infiltrating but benign tumor of neural sheath origin, most commonly found in the tongue or integument, although approximately 7% involve the vulva. The usual picture consists of small subcutaneous nodules 1–4 cm in diameter. With increasing size, they erode through the surface and result in ulcerations that may be confused with cancer. The margins of the tumor are indistinct, and wide local excision is necessary to completely excise the cells extending into contiguous tissues. The area of resection must be periodically re-examined and secondary excision performed promptly if recurrence is suspected
Vulvar Pain Syndrome • Vulvar pain in the absence of relevant, visible physical findings is termed vulvodynia. • The patient suffering from vulvodynia describes her symptoms as burning, rawness, irritation, dryness, and hyperpathia (pain provoked by very light touch). • Approximately 16% of the female population has experienced vulvodynia and approximately 1.5% currently suffer from the disorder. • Vulvodynia has been classified into generalized vulvodynia (provoked or unprovoked) and localized vulvodynia (provoked and unprovoked). • a detailed history and examination are important to help determine the etiology and to direct the diagnosis and treatment.
Vulvar Pain Syndrome-Etiology • Infections • Bartholin's gland abscess, vulvovaginal candidiasis, herpes, herpes zoster, human papillomavirus, molluscum contagiosum, trichomoniasis • Trauma • Sexual assault, prior vaginal deliveries, hymenectomy • Systemic Illness • Behçet's disease, Crohn's disease, Sjögren's syndrome, systemic lupus erythematosus • Neoplasia • Vulvar intraepithelial neoplasia and invasive squamous cell carcinoma
Vulvar Pain Syndrome-Etiology • Allergens/toxic medications • Soaps, sprays, douches, antiseptics, suppositories, creams, laser treatment, podophyllin, trichloroacetic acid, 5-fluorouracil • Dermatologic conditions • Allergic and contact dermatitis, eczema, hidradenitis suppurativa, lichen planus, lichen sclerosus, pemphigoid, pemphigus, psoriasis, squamous cell hyperplasia • Urinary tract syndromes • Interstitial cystitis and urethral syndrome
Vulvar Pain Syndrome-Etiology • Neurologic • Referred pain from urethra, vagina, and bladder; • dysesthesias secondary to herpes zoster, spinal disk problems; • specific neuralgias (pudendal, genitofemoral) • Psychological • Sexual/physical abuse history
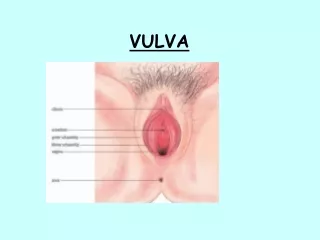
Localized Provoked Vulvodynia • was formerly known as vulvar vestibulitis/clitorodynia. • The vestibule is the nonpigmented, nonkeratinized squamous epithelium of the vulva between the labia minora and the hymen • generally affects women in their 20s and 30s who complain of introital dyspareunia. • present as persistent vaginal discharge and burning. • is characterized by 3 criteria: • introital pain on vestibular or vaginal entry (entry dyspareunia), • vestibular erythema or inflammation of the vestibule, commonly involving the posterior fourchette, and • vestibular tenderness—pressure from a cotton-tipped applicator at the vestibule reproduces the pain.
Localized Provoked Vulvodynia • Patients should be instructed on proper vulvar hygiene (cotton underwear, keeping area dry, avoidance of constrictive garments and irritating agents). • The initial conservative approach to therapy includes topical estradiol with twice-daily application, 5% lidocaine ointment daily, calcium citrate 400 mg 3 times daily to decrease the urinary oxalate crystal concentration, oral antifungal therapy using fluconazole 150 mg weekly, and pelvic floor therapy with biofeedback.
Localized Provoked Vulvodynia • The injectable forms of therapy include intralesional interferon injection to treat possible HPV, trigger point injections with long-acting injectable anesthetics, and injection of botulism toxin to treat vaginismus as the source of vulvodynia. • The surgical treatment of localized provoked vulvodynia in the form of vulvar vestibulectomy with vaginal advancement is most effective (70% success rate) in patients who have been refractory to more conservative therapies.
Generalized Unprovoked Vulvodynia • was formerly known as pudendal neuralgia. • Its etiology is unknown. • The pain involves a larger surface area than that of localized vulvodynia. • The average patient is in her 40s. • The typical patient complains of intermittent or constant burning sensation with periods of unexplained relief and/or flares. The diagnosis is made by exclusion. • Infections and dermatosis should be ruled out.
Generalized Unprovoked Vulvodynia • A test for allodynia and hyperalgesia using a cotton-tipped swab should be performed. • It is believed to be a neuropathic pain, but other organic causes, including pudendal nerve entrapment, pudendal nerve injury due to child birth, referred pain from ruptured disk, neuropathic viruses such as herpes simplex or varicella-zoster, and neurologic disease such as multiple sclerosis, are possible.
Generalized Unprovoked Vulvodynia • Treatment of generalized unprovoked vulvodynia is mostly unsuccessful. • The patient should be counseled on elimination of irritants and on self-care. • Topical local anesthetics, tricyclic antidepressants, or anticonvulsants such as gabapentin can be tried. • If the patient is refractory to such treatment, acupuncture or referral to a pain center may be attempted.
BENIGN DISORDERS OF VAGINA Rukset Attar, MD, PhD Department of Obstetrics and Gynecology
Benign Disorders of Vagina • Vulvovaginitis • Benign cysts • Congenital anomalies • Mullerian anomalies • Hymenal Septum • Hymen imperforatus