Download
1 / 21
250 likes | 784 Views
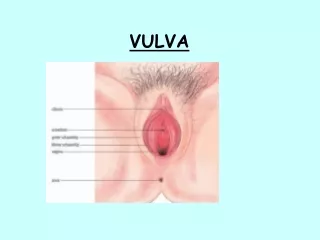
Lesions of the Vulva. Pediculosis pubis. Phthirus pubis Body louse Obtained from Close contact Towels, beddings Located near the hair shaft of hair Can lodge in the vulva, eyelids Eggs deposited in the base of the hair follicles Constant itching of the perineal area

E N D
Pediculosis pubis • Phthirus pubis • Body louse • Obtained from Close contact • Towels, beddings • Located near the hair shaft of hair • Can lodge in the vulva, eyelids • Eggs deposited in the base of the hair follicles • Constant itching of the perineal area • Incubation period: 30 days • Nourished by human blood
Diagnostics: Scratch skin papule adjacent to hair shaft and place under a drop of mineral oil (Eggs, lice, pepper-grain feces) • Treatment : Must kill both the adult parasite and egg: • Permethrin 1% (Kwell) shampoo (Don’t let it enter the eyes!) • Apply for 5 minutes then wash off thoroughly • Avoid eyelids
Scabies • Sarcoptesscabiei • Close contact • Widespread doesn’t spare the vulva • Adult female digs a burrow underneath the skin • Travels about 2.5 cm/min • Severe but intermittent itching exacerbated at night • Papules, vesicles, or burrows • The great dermatologic imitator because aside from itching, it can produce other skin problems • Treatmentsame as Pediculosis • Permethrin cream 5% • Applied to all areas of the body, from neck down, wash off after 8-14 hours • Household contacts: Treat patient and the rest of the household because you can get it from bedding, fomites or close contact. This should include treating house help. • Decontaminate beddings and clothing by hot washing.
Molluscumcontangiosum • Pox virus • Papules with umbilicated center • Characteristic crater in the middle. • 1-5 mm (Not very big) • 1 to 20 solitary lesions randomly distributed over the vulvar skin.
new nodules will persist from several months to years. • Skin-to-skin contact • Incubation: 2-7 weeks • Self-limiting, mildly contagious in immunocompetent persons • Replicates in cytoplasm
Condylomaacuminatum • CondylomaAcuminatum • Genital, venereal, or anogenital warts, • Human Papilloma Virus • Most common viral STD of the vulva, vagina, rectum and cervix • >70 HPV subtypes • pinhead-sized papules to large cauliflower-like masses. • usually asymptomatic • Some are symptomatic: pain, itching, tendency to bleed when friable • Associated with other infections • Type 6, 11: Associated with benign genital tract lesions • Types 16, 18: Associated with pre-malignant or malignant lesions
Predisposing factors: • Immunosuppression • Diabetes • Pregnancy • Trauma • Treatment: • Depends on size, location and pregnancy • If only a few lesions: chemical, electrocautery, immunotherapy
Chemical • Patient administered: Imiquimod 5% cream (Aldara) • Immune enhancer • Daily, at bedtime, up to 16 weeks • Wash 6-10 minutes • Another option is Interferon. However, this is very expensive and is only available in western countries. • Provider-administered: • Cryotherapy • Electocautery • Podophyllin (weekly): applied by physician • Trichloroacetic Acid (TCA) weekly
Syndromic management of STIs • Public health approach • Prevention and promotion take precedence • Population perspective • Cost-effectiveness
Syndromic Management of STIs • Case and point: Puerto Galera • Hospitality industry • Not all use condoms • MHO sends midwives to check on women weekly • Checkup necessary to renew “hospitality permit” • 2 MHOs for the whole town; undermanned • Expenses are out-of-pocket
Approaches to STI diagnosis • Etiological diagnosis • Clinical diagnosis • Syndromic case management
Syndromic approach • Steps: • history-taking and examination • diagnosis and treatment, using flowcharts • counseling and education on safer sex, including condom promotion and provision • partner management • data gathering (recording)
Syndromic approach • problem-oriented (patient’s symptoms) • highly sensitive and does not miss mixed infections • treats the patient at the first visit • makes STI care more accessible • (primary care level) • uses flowcharts • provides opportunity and time for education and counseling
Criticisms • Unscientific • Similar diagnostic accuracy as clinical diagnosis • Too simple for physicians • Should be simple enough to be used by a primary healthcare worker • More time for education and behavior change • Fails to make sure of clinician’s skills and experience • Clinicians using own clinical judgement misdiagnose 50% of the time
Treating for most common cause then treat for second cause if symptoms don’t improve • Most patients don’t return to health center • Patient will continue to transmit STI • Waste of drugs because of overtreatment • Studies show that syndromic approach is less expensive