Download
1 / 80
830 likes | 1.3k Views
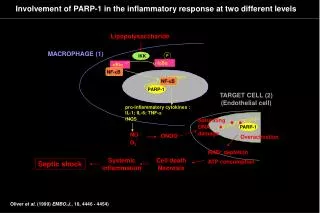
Nonsteroidal Anti-inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopioid Analgesics, & Drugs Used in Gout Dr. Florencia D. Munsayac. The Inflammatory Response. 3 Phases of Inflammation: Acute Inflammation The Immune Response Chronic Inflammation.

E N D
Nonsteroidal Anti-inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopioid Analgesics, & Drugs Used in GoutDr. Florencia D. Munsayac
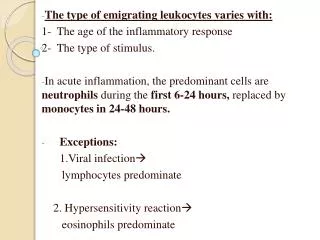
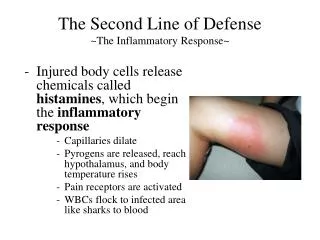
The Inflammatory Response 3 Phases of Inflammation: • Acute Inflammation • The Immune Response • Chronic Inflammation
Therapeutic Strategy 2 Primary Goals: • The relief of pain - NSAIDs - Nonopioid analgesics - Corticosteroids • The slowing or--in theory--arrest of the tissue damaging process - SAARDs or DMARDs
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS 8 Groups of NSAIDs: • Salicylic acid derivatives (Aspirin, Na salicylate, choline Mg++ trisalicylate, salsalate, diflusinal, sulfasalazine) • Para-aminophenol (Acetaminophen) • Para-chlorobenzoic acid derivatives or indoles (Indomethacin, Sulindac) • Pyrazolone derivatives (Phenylbutazone) • Arylpropionic acid (Ibuprofen, Flurbiprofen, Ketoprofen, Fenoprofen, Naproxen, Oxaprozin) • Fenamates/Anthranilic acids (Mefenamic Acid, Meclofenamic acid) • Enolic acids/Oxicams (Piroxicam, Meloxicam) • Heteroaryl/Penylacetic acids (Diclofenac Sodium, Tolmetin, ketorolac) • Alkalones (Nabumetone) • Selective COX-2 inhibitors (Celecoxib, Rofecoxib, Etodolac, Nimesulide)
SALICYLATES • Aspirin or Acetylsalicylic Acid (ASA) • Comes from the family of salicylates derived from salicylic acid • Prototype drug • Developed in 1899 by Adolph Bayer • The oldest anti-inflammatory agent
SalycilatesPharmacokinetics • Rapidly absorbed from the stomach & upper small intestine • Peak plasma level: 1-2 hrs • 80-90% protein bound • t1/2: 3-5 hrs • Cross BBB & placental barrier • Undergoes hepatic metabolism • Excretion: kidneys
SalycilatesPharmacodynamics . MOA: - Inhibits prostaglandin synthesis - Irreversibly blocks the enzyme cyclooxygenase (PG synthase) . Pharmacological Properties & Therapeutic indications: - anti-inflammatory effects - analgesic effects - antipyretic effects - Platelet effects - Uricosuric effects . Dosage: children: 50-75mg/kg/day adult: 325-650mg p.o. q 4 hrs
SalicylatesAdverse Effects • Gastric upset • Salicylism vomiting, tinnitus, decreased hearing, & vertigo • Hyperpnea • Respiratory alkalosis later acidosis supervenes • Glucose intolerance • Carditoxicity • Increases uric acid levels • Elevation of liver enzymes, hepatitis, decreased renal function, bleeding, rashes, asthma • Reye’s syndrome
SalicylatesContraindications • Pregnancy • Severe hepatic damage • Vitamin K deficiency • Hypoprothrombinemia • Hemophilia • PUD • Viral (chickenpox & influenza)
Special Drug Characteristics or NonAcetylated Salicylates • Sodium salicylate, sodium thiosalicylate, Mg salicylate & choline salicylate • Salisalicylate • Methylsalicylate (oil of wintergreen) • Diflunisal
ACETAMINOPHEN • Active metabolite of phenacetine • A weak PG inhibitor • No significant anti-inflammatory effect • For the treatment of mild to moderate pain • Antipyretic effect
AcetaminophenPharmacokinetics • Administered orally • Absorption: related to rate of gastric emptying • Peak blood conc: 30-60 min • Slightly protein bound • Partially metabolized by hepatic microsomal enzyme acetaminophen SO4 & glucuronide • Excretion: unchanged < 5% • A minor but highly active metabolite (N-acetyl-p-benzoquinone) is important liver & kidney toxicity • t1/2: 2-3 hrs
AcetaminophenIndications • HA, myalgia, postpartum pain • ASA allergy, hemophilia or hx of PUD, bronchospasm precipitated by ASA, & children with viral infection • Analgesic adjunct to anti-inflammatory therapy • Gout
AcetaminophenAdverse Effects • Mild increase in hepatic enzymes • Dizziness, excitement & disorientation • Ingestion of 15gm: fatal death caused by hepatotoxicity with centrilobular necrosis & sometimes with acute renal tubular necrosis • Symptoms of early hepatic damage: N/V, diarrhea, abdominal pain • Antidote: acetylcysteine (sulfhydryl groups) • Caution: liver disease • Dosage: 325-500mg q.i.d.
INDOMETHACIN • Introduced in 1963 • An indole derivative • A more potent analgesic, antipyretic & anti-inflammatory agent than ASA • Nonselective COX inhibitor • May also inhibit phospholipase A & C • Reduce PMN migration • Decrease T & B cells proliferation
IndomethacinPharmacokinetics • Rapidly & almost completely absorbed from GIT • Peak concentration: 2 hrs • Metabolism: liver & extensive enterohepatic circulation • Excretion: bile, urine, feces
IndomethacinDrug Interaction • Probenecid • Furosemide • Thiazide • Beta adrenergic blocking agents
IndomethacinTherapeutic Uses • Rheumatic conditions • Gout & ankylosing spondylitis • Patent ductus arteriosus • Sweet’s syndrome • Juvenile rheumatoid arthritis • Pleurisy • Nephrotic syndrome • Tocolytic agent
IndomethacinAdverse Effects • Gastrointestinal effects (abdominal pain, diarrhea, GI hemorrhage, pancreatitis) • Headache, dizziness, confusion, depression • Psychosis with hallucination • Thrombocytopenia • Aplastic anemia • hyperkalemia
IndomethacinContraindications • Nasal polyps • Angioedema • Asthma • Renal failure • Enterocolitis • hyperbilirubinemia
SULINDAC • A sulfoxide prodrug • An acetic acid derivative • Reversibly metabolized to active metabolite sulfide more potent as cyclooxygenase inhibitor , enterohepatic recycling prolongs DOA: 12-16 hrs, excreted in bile • Metabolized to an inactive sulfone
SulindacPharmacokinetics • 90% absorbed after oral administration • Peak concentration: 1 hr • t1/2: 7 hrs • First pass kinetics
SulindacTherapeutic Indications • Rheumatoid arthritis • Suppresses familial intestinal polyposis • Ankylosing spondylitis • Osteoarthritis • Acute Gout • Tocolytic agent
SulindacAdverse Effects • GI side effects: abdominal pain & nausea • CNS side effects: drowsiness, dizziness, HA, nervousness • Skin rash & pruritus • Transient elevations of hepatic enzymes
TOLMETIN • A nonselective COX inhibitor • Effective anti-inflammatory with analgesic & antipyretic effects • Has a short half-life: 5 hrs • Given frequently not often used • Ineffective in gout unknown • SE: allergic IgM-related thrombocytopenic purpura, GI & CNS effects
DICLOFENAC • A simple phenylacetic acid derivative • A potent nonselective cyclooxygenase inhibitor • Decreases arachidonic acid bioavailability • Has the usual anti-inflammatory, antipyretic & analgesic properties
DiclofenacPharmacokinetics • Rapidly absorbed following oral administration • 99% protein bound • 30-70% systemic bioavailability first pass hepatic metabolism • t1/2: 1-2 hrs • Accumulates in synovial fluid t1/2 of 2-6 hrs • Metabolized by CYP3A4 & CYP2C9 • 30% biliary clearance, urine (65%)
DiclofenacAdverse Effects • GI distress • Occult GI bleeding • Gastric ulceration • Elevates serum aminotransferases Preparations: ophthalmic, dermatologic, IM administration
ETODOLAC • A racemic acetic acid derivative • Slightly more COX-2 selective, with COX-2:COX-1 activity ratio of 10 • Clinical uses: postoperative analgesia, osteoarthritis, rheumatoid arthritis • SE: GI irritation & ulceration (less)
EtodolacPharmacokinetics • Rapidly well absorbed • 80% bioavailability • Strongly bound to plasma proteins (99%) • Enterohepatic circulation • t1/2: 7 hrs • Dosage: 400-1600mg/d • Excreted in the urine
KETOROLAC • Potent analgesic with moderate anti-inflammatory & antipyretic effects • Inhibits platelet aggregation • Promotes gastric ulceration & renal impairment • Indications: postsurgical pain, chronic pain, inflammatory conditions of the eye, seasonal allergic conjunctivitis topical
Pharmacokinetics • Rapidly absorbed after oral or IM administration • Also given IV • Peak concentration: 30-50 min. • 80% oral bioavailability • Almost totally protein bound • t1/2: 4-6 hrs • Metabolized to active & inactive forms • Excreted in the urine (90%)
FENOPROFEN • A propionic acid derivative • t1/2: 2-4 hrs • Given q.i.d. • Toxic effect: interstitial nephritis • Adverse effects: nephrotoxicity, nausea, dyspepsia, peripheral edema, rash, pruritus, CNS & CVS effects and tinnitus
FLURBIPROFEN • A propionic acid derivative • Inhibits COX nonselectively • Also affect TNF-a & nitric oxide synthesis • t1/2: 0.5-4 hrs • Extensive hepatic metabolism • Dosages: 200-400mg/day • Ophthalmic formulation inhibition of intraoperative miosis • SE: GI symptoms, cogwheel rigidity, ataxia, tremor & myoclonus
IBUPROFEN • A simple derivative of phenylpropionic acid • Dose: 2400mg daily • 99% protein bound • Rapidly cleared • Terminal t1/2: 1-2 hrs • Extensively metabolized in CYP2C8 & CYP2C9 in the liver • SE: GI irritation & bleeding • CI: nasal polyps, angioedema, bronchospastic reactivity to ASA, rash, pruritus, tinnitus, dizziness, HA, aseptic meningitis, fluid retention, agranulocytosis, aplastic anemia, ARF, interstitial nephritis, nephrotic symdrome
KETOPROFEN • A propionic acid derivative • Inhibits both cyclooxygenase (nonselective) & lipoxygenase • Rapidly absorbed • Elimination t1/2: 1-3 hrs • Metabolized in the liver (glucuronide) • DI: probenicid • Dosage: 100-300mg/day • Indication: RA, OA, GA, dysmenorrhea • AE: GIT & CNS
NAPROXEN • Is a naphthylpropionic acid • A nonselective COX inhibitor • Elimination serum t1/2: 12 hrs • High albumin binding • Metabolism: CYP2C9, less in CYP1A2 & CYP2C8 • Prep: SR formulation, oral susp • AE: UGIB, allergic pneumonitis, leukocytoclastic vasculitis, & pseudoporphyria
OXAPROZIN • a propionic acid derivative • t1/2: 50-60 hrs • Does not undergo enterohepatic circulation • Given o.d. • Is a mild uricosuric agent
PIROXICAM • An oxicam • A nonselective COX inhibitor • Also inhibits PMN leukocyte migration, decreases O2 radical production, & inhibits lymphocyte function • Mean t1/2: 50-60 hrs • Dosing: o.d. or every other day
PiroxicamPharmacokinetics • Rapidly absorbed from the stomach & upper intestine • Peak plasma concentration: 1 hr • Extensively metabolized to inactive metabolites • 99% protein bound • Elimination: renal – 5% unchanged • Toxicity: GI symptoms, dizziness, tinnitus, HA & rash, increased incidence of PUD and bleeding
MELOXICAM • An enolcarboxamide • Slightly COX-2 selective • Slowly absorbed • t1/2: 20 hrs • Clearance: 40% decreased in elderly • Dose: 7.5-15mg/d for RA & OA • Slightly less ulcerogenic
NABUMETONE • The only nonacid NSAID • Converted to the active acetic acid derivative in the body • Given as a ketone prodrug • t1/2: > 24 hrs • Deos not undergo enterohepatic circulation • Cause less gastric damage • Cause pseudoporphyria & phosensitivity
PHENYLBUTAZONE • A pyrazolone derivative • Withdrawn from the market in North American & most European markets • Toxicity: aplastic anemia agranulocytosis
MECLOFENAMATE & MEFENAMIC ACID • Fenamic acid derivatives • Inhibit both COX & phospholipase A2 • Peak plasma level: 30-60 min • t1/2: 1-3 hrs • SE: LBM, abdominal pain (meclofenamate) • CI: pregnancy, children • DI: oral anticoagulants
CELECOXIB • Highly selective COX-2 inhibitor • Absorption: 20-30% decreased by food • t1/2: 11 hrs • Highly protein bound • Metabolized by CYP2C9 • Clearance affected by hepatic impairment • Effective dose: 100-200mg b.i.d. • Does not affect platelet aggregation • DI: warfarin • AR: dyspepsia