Download
1 / 32
320 likes | 541 Views
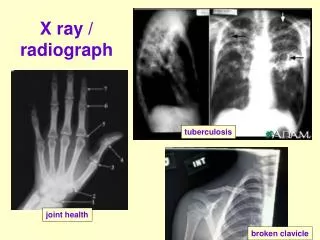
Radiograph Interpretation Basics. How X-rays are made. X-ray tube produces ionizing radiation Ionization can be damaging to tissues, especially when gonads, thyroids, and eyes are irradiated

E N D
How X-rays are made • X-ray tube produces ionizing radiation • Ionization can be damaging to tissues, especially when gonads, thyroids, and eyes are irradiated • Consider that the fetus is most radiosensitive during organogenesis (2nd-8th week) when ordering abdominal exams on females • Different tissue types attenuate/absorb radiation differently (air-dark, fluid/soft tissue-gray, bone-white)
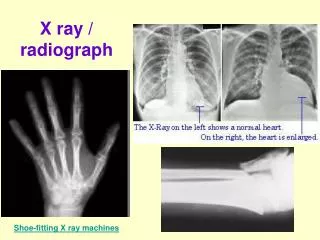
Chest X-rays • Most frequently performed exam • Provides important information about soft tissues, bones, lung tissue, pleura and mediastinum • Standard patient position is PA and left lateral (both of these place heart closest to the film) • Upright for air-fluid levels • 72” distance to reduce heart magnification
Normal Chest x-rays • Costophrenic and cardiophrenic angles • Right hemidiaphragm will be 1-2 cm higher than left • Compare lung size and radiolucency • Full inspiration – should see 10 posterior ribs with thoracic vertebrae faintly visible through mediastinum • Trachea in the midline
Normal Chest x-rays • Various soft tissue densities are present • Pectoral muscles overlie and extend beyond lung fields • Breast shadows are in mid chest region (females may overlie costophrenic angles) • Nipple shadows may be visible (can do chest obliques with nipple markers to discern whether nipple or nodule) • Mediastinum – heart occupies large portion – transverse diameter < ½ thorax diameter
Chest Pathologies • Normal Chest – heart size < ½ thorax diameter • Cardiomegaly with CHF – pulmonary edema around hila with hilar vessels engorged. Heart > ½ thorax diameter • Pneumothorax – presence of air in the pleural cavity leading to complete or partial lung collapse. Hyperradiolucent area without lung markings. Due to obstruction, penetrating trauma or spontaneous. If entire lung collapses, mediastinum may shift toward affected side.
Chest Pathologies • Atelectasis – collapse of alveoli ->diminished air in an area of the lung. Shown as a plate-like area of increased density usually. Caused by air or fluid in the pleural space, bronchial obstruction, tumor outside lung, improper placement of ET tube • ET tubes, if incorrectly placed, are likely to go into the right primary bronchus, so it blocks the left primary bronchus, causing its collapse
Chest Pathologies • Pleural effusion (fluid in the pleural cavity) or Pulmonary edema (fluid accumulation in lungs) • Can be seen during upright cxr, also is shown on lateral decubitus views (a must for patients who cannot sit up or stand) • Emphysema • Barrel chest, flattened diaphragm, elongated lung fields.
Chest Pathologies • Pneumonia – • Primary Lung CA – (bronchogenic carcinoma – most common primary lung malignancy in US) • If you see a chest nodule: • Look for old films ( > 1 yr) for comparison • Look for calcifications (calcifications generally are benign) • Look for irregular margins • CT chest w/wo contrast is the next imaging step
Chest Pathologies • Metastatic Lung CA – can have “cottonball” effect. • Hyaline Membrane Disease (IRDS – idiopathic respiratory distress syndrome) – “ground glass” appearance caused by underaeration, uninflated alveoli. Lungs appear dense due to lack of air • ET tube should be at level of clavicle
Chest Pathologies • Histoplasmosis – fungal infections from dust of bird droppings, seen in older, rural patients • Sarcoidosis – may look similar to histoplasmosis • 1. perihilar density – lymph nodes enlarged • 2. diffuse interstitial pattern, coarse lung markings throughout both lungs, sometimes with small, larger widely scattered granulomatous nodules.
Chest Pathologies • Silicosis – a pneumoconiosis from inhaling silica sand, leads to fibrosis
Abdomen • KUB – taken prior to contrast exams to rule out pathology/improper exam prep • See liver, kidneys, bowel gas, abnormal masses, calcification, and foreign bodies
Abdomen • An acute abdominal series includes: • Supine KUB – “flat plate” • Upright KUB – looking for intraperitoneal air and/or air/fluid levels • Upright PA chest – also looking for free air • And is ordered for suspected acute or emergency conditions like bowel obstruction, perforations, intra-abdominal masses, situsinversus
Upper GI • Shows hiatal hernias (stomach above diaphragm), gastric ulcers (crater fills with barium) • Requires patient to drink barium
Barium Enema/Lower GI • Barium is inserted through the rectum • Can shows ulcerative colitis, Crohn’s disease, colon cancer, diverticula, polyps, etc. • Fewer Barium Enemas are being done • Getting colonoscopies, virtual (CT) colonoscopies
Small Bowel • Patient drinks barium – should show from duodenum all the way to terminal ileum • Shows Crohns disease well • May take up to 6 hours for the barium to progress from mouth to cecum
IVP/IVU • Iodinated contrast is injected intravenously and picked up by the kidneys • Patients who have compromised renal function may suffer deleterious effects from the contrast • If looking for renal calculi only, most places can perform a CT –Renal Stone protocol without using contrast • Can show hydronephrosis, renal calculi, etc. • VERY few of these are being done in this area
Bony Pathologies • Osteoporosis – often an incidental finding on other exams • Bone metastasis • MRSA • Fractures • Colles – distal radius fx, caused by falling on an outstretched arm • Comminuted - splintered
Bony Pathologies • Cervical spine • Lateral shows alignment • Should see all 7 vertebrae in lateral C-spine film • Lumbar spine • Osteoporosis – bone is less dense • Spondylolithesis – one vertebrae slips forward on another • Bone mets • Multiple myeloma
Imaging modalities • Sonography • Nuclear Medicine • Mammography • CT • MRI
Sonography • Pros • Ionizing radiation not used • Relatively inexpensive • Cons • Visualization may be difficult with • Lots of bowel gas • Obesity/Overweight patients
Nuclear Medicine • Pros • Bone scans (osteomyelitis/bony mets/occult fractures) • VQ scans for PE if CT can’t be used • Cons • Uses radioactivity • Injections/oral dosing may be inconvenient
Mammography • Less helpful with dense breast tissue (usually seen in younger women) • More helpful for solid masses while breast sonography is better for cystic masses
CT • Pros – fast, shows many body parts well, not as influenced by body size as other modalities • Cons – radiation dose, obese patients may not fit through the gantry or may exceed weight limits (depends on facility – average around 400 pounds)
MRI • Pros – great for soft tissue and detail • Cons – certain patients can’t be scanned (those with certain metals, pacemakers, etc.) • Claustrophobic patients may be scanned under anesthesia • LONG! • Not good for areas with high motion (orbits, abdomen)
CT vs. MRI • Most bone issues – order a CT • For most joint issues (ligaments, tendons) – order MRI • Abdomen and Pelvis – order a CT • MS – MRI • Chest – CT • Spines – MRI (CT okay post myelogram) • Head exams – order CT unless… • Tumor followup, very fine detail (pituitary) then MRI
Contrast • Rules of thumb • Very few head CTs need contrast • Tumor followup, MS (although MRI is better), infections, and known mets will probably use contrast • CT Soft tissue necks always use contrast • Chest CT – use contrast if cancer/staging (otherwise unnecessary for screening, nodules, etc)
Contrast • Most Abd/Pelv will use oral contrast and IV contrast • Renal stone protocols use NO contrast • CT Spines – don’t use contrast • IV contrast is the ONLY way to see vessels in CT (MRAs don’t require contrast) • MRI spines – use contrast if they’ve had surgery on spine before • If you’re looking for an infection, use contrast
Contrast • Oral contrast takes approx 2-3 hours for complete transition if done as a work in patient before we can scan them. They drink approx 900ml of contrast. Oral contrast is used in CT • Enterography is ordered to look at the small bowel and the patient has to prep at the hospital the morning of. • If patients are allergic to contrast they need to be premedicated for possible reaction, recommendation of protocol to use is in the radiology department and can be asked for. • If the patient has had a break through reaction (reaction after being premed) they will not receive IV contrast again.
Contrast info • Prep instructions are given to office at time of scheduling, rule of thumb IV contrast is NPO four hours prior minimum whether CT or MR. If oral contrast is needed some offices stock this or the patient has to go to the respective imaging department to pick this up the day before the appointment. • When looking for a structure that lies within the abdominal cavity if any of that structure( such as colon) lies below the umbilicus then a Pelvis order is also needed. • Can scan pelvis for bony detail only if for trauma • Biggest thing is to make sure to include the diagnosis or what you’re looking for on the order so we can make sure the correct protocol is used. • If venous access is issue or allergy a VQ scan(nuc med study) can be done instead of a PE study
Misc. • http://www.med.yale.edu/intmed/cardio/imaging/contents.html • Questions???