Download
1 / 34
570 likes | 1.44k Views
The Basics of ECG Interpretation. Dr Tim Smith. Summary. Cardiac conducting system and the ECG waveform The normal ECG Abnormalities of conduction Heart Rhythms QT prolongation Normal Variants. Cardiac Depolarisation. Originates in pacemaker cells (automaticity).

E N D
The Basics of ECG Interpretation Dr Tim Smith
Summary • Cardiac conducting system and the ECG waveform • The normal ECG • Abnormalities of conduction • Heart Rhythms • QT prolongation • Normal Variants
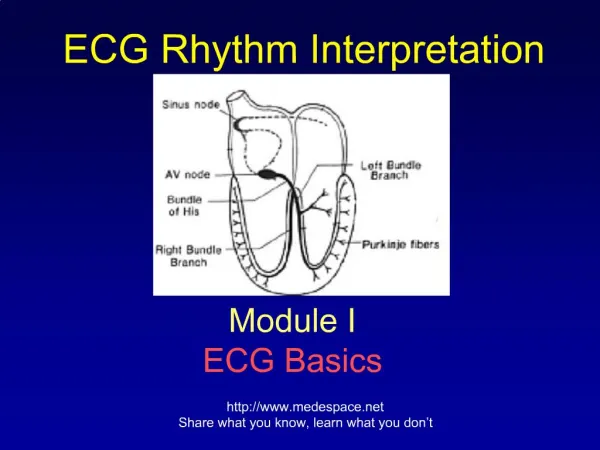
Cardiac Depolarisation • Originates in pacemaker cells (automaticity). • Spreads along defined pathways. • Causing co-ordinated muscular contraction. • Electrical signal from depolarisation detectable at body surface. (1 mV cf. 90 mV @ cell) • This is the ECG.
The Limb Leads • I, II, VL - L lateral surface • VF, III - Inferior surface • VR - R atrium • Cardiac Axis • Lead II often used for rhythm strips.
The Chest Leads • V1+2 - R Venticle • V3+4 - Septum • V5+6 - L Ventricle • Bundle Branch Blocks • Ischaemia (esp. V5)
Characteristics of the Normal ECG • Rate 50-100 bpm • Sinus rhythm • Cardiac Axis -30º to +90º • P <120 ms • PR <200 ms • QRS <120 ms • QT Male <0.43 s Female <0.45 s • ST isoelectric
Calculating Heart Rate • Standard ECG speed is 25 mm.s-1 • Heart Rate = 300/# big squares 300/3.8=79 bpm
Abnormalities of conduction • At the AVN = Heart Block • 1st degree • 2nd degree • 3rd degree • In the His/Purkinje system = Bundle Branch Block • LBBB • RBBB
First Degree Heart Block • Prolonged PR interval >200 ms (5 small sq.) • Slow conduction through the AVN • Not itself important • May indicate disease: • RA • IHD • Dig. Toxicity
Second Degree Heart Block Mobitz Type I (Wenkebach) • Increasing PR interval preceding unconducted P. • Does not usually cause symptoms. • May indicate disease (RA, IHD, Dig.). • Usually benign
Second Degree Heart Block Mobitz Type II • Fixed PR interval with some unconducted P waves. • May occur with fixed ratio eg. 2:1 block • Indicates underlying disease. • May cause symptoms/precede complete block.
Third Degree (Complete) Heart Block • No relationship between P & QRS • QRS often wide • Atrioventricular dissociation • Impairs cardiac performance.
Left Bundle Branch Block • Characteristic, widened QRS in chest leads • Will not cause symptoms itself • Always indicates underlying heart disease • Makes ECG interpretation difficult or impossible W i LL ia M
Right Bundle Branch Block • Characteristic, widened QRS in chest leads • May indicate right heart disease • Can occur in normal individuals • Partial RBBB is always normal. M a RR o W
Heart Rhythm Always ask: • What is the QRS width? • <120ms => Supraventricular source • >120 ms => Ventricular source (or BBB) • Is there a P wave? • Is the rhythm regular/irregular/irregularly irregular?
Supraventricular Rhythms (1) • Normal Sinus Rhythm
Supraventricular Rhythms (2) • (Respiratory) Sinus Arrhythmia Inspiration Expiration
Supraventricular Rhythms (3) • Supraventricular Ectopic
Supraventricular Rhythms (4) • Junctional Escape Beat
Supraventricular Rhythms (5) • Sinus Tachycardia
Supraventricular Rhythms (6) • Junctional Tachycardia
Supraventricular Rhythms (7) • Atrial Fibrillation
Supraventricular Rhythms (8) • Atrial Flutter
Ventricular Rhythms (1) • Ventricular Ectopic and Couplet
Ventricular Rhythms (2) • Ventricular Bigeminy
Ventricular Rhythms (3) • Ventricular Tachycardia
Ventricular Rhythms (4) • Ventricular Fibrillation
QT Prolongation • QT represents the ventricular refractory period • Normal <450 ms (ish) • Risk of prolongation... Torsades de Pointes - potentially lethal.
QT Prolongation • ? How long is too long • Affected by temperature, gender, heart rate • Diurnal variation up to 70 ms • Numerous drugs: • Cisapride • Terfenadine • Total of 48 listed as causing TdP by FDA
Normal Variants • Always normal: • Sinus Arrhythmia • Supraventricular Extrasystoles • Partial RBBB • Often normal: • Sinus Bradycardia (and pauses in athletes) • First Degree Heart Block • Ventricular Extrasystoles • Left/Right Axis Deviation • RBBB