Download

1 / 15
150 likes | 264 Views
Design and baseline characteristics. Trial hypothesis. SIGNIFY is assessing whether heart rate reduction using ivabradine improves cardiovascular mortality and morbidity in patients with stable CAD, without clinical heart failure. Fox K et al. Am Heart J. 2013;166(4):654-661.

E N D
Trial hypothesis SIGNIFY is assessing whether heart rate reduction using ivabradine improves cardiovascular mortality and morbidity in patients with stable CAD, without clinical heart failure Fox K et al. Am Heart J. 2013;166(4):654-661.
Target population • Proven stable CAD • Age >55 years • Without LVSD (EF >40%, no clinical signs of HF) • In sinus rhythm, with a resting heart rate >70 bpm • Receiving appropriate and stable doses of conventional cardiovascular medication • With one or more other cardiovascular risk factors Fox K et al. Am Heart J. 2013;166(4):654-661.
Additional cardiovascular risk factors (1) • At least ONE major risk factor: • Angina pectoris in CCS class II or higher (≥1 mo); or • Objective evidence of myocardial ischemia with moderate to large deficit induced by noninvasive stress testing (≤12 mo) without subsequentrevascularization; or • Hospital discharge after coronary event ≤12 mo (AMI >3 mo or UA >1 mo) Fox K et al. Am Heart J. 2013;166(4):654-661.
Additional cardiovascular risk factors (2) • OR at least TWOminor risk factors: • Low HDL-C (<40 mg/dL) and/or high LDL-C (<160 mg/dL) despite lipid-lowering treatment; or • Type 1 or 2 diabetes mellitus; or • Peripheral artery disease; or • Current smoker (≥10 cigarettes/d); or • Age ≥70 years Fox K et al. Am Heart J. 2013;166(4):654-661.
Multinational study • 19 102 patients, 51 countries, 1139 centers Fox K et al. Am Heart J. 2013;166(4):654-661.
Executive CommitteeK. Fox chair, R. Ferrari co-chair I. Ford, P.G. Steg, J-C Tardif, M. Tendera SteeringCommittee V. Chumburidze (Georgia) T. Münzel (Germany) P. Vardas (Greece) J. Borbola (Hungary) R. Kasliwal (India) P. Crean (Ireland) L. Tavazzi (Italy) T.Z. Seisembekov (Kazakhstan) K.B. Seung (Korea) A.Erglis (Latvia) A. Laucevicius (Lithuania) R. Ali (Malaysia) E. Alexanderson (Mexico) D. Atar (Norway) R. Sy (Philippines) A. Rynkiewicz (Poland) R. Seabra-Gomes (Portugal) C. Macarie (Romania) V.Y. Mareev and Y.A. Karpov (Russia) R. Ferrari (Chair, Ferrara, Italy) R. Iglesias (Argentina) P.A. Zelveian (Armenia) B. Freedman (Australia) K. Huber (Austria) J-L.Vanoverschelde (Belgium) L.A. Machado Cesar (Brazil) N. Gotcheva (Bulgaria) P. L’Allier (Canada) D.Y. Hu (China) C.P. Lau (Hong Kong) M. Bergovec (Croatia) J. Hradec (Czech Republic) P. Clemmensen and P. Hildebrandt (Denmark) J. Eha (Estonia) M. Laine (Finland) N. Danchin (France) S. Kedev (FYROM) M.C. Ostojic (Serbia) T.H. Koh (Singapore) J. Murin (Slovakia) P. Rakovec (Slovenia) P. Sareli (South Africa) C. Macaya (Spain) M. Dellborg( Sweden) T. Lüscher (Switzerland) C.E. Chiang (Taiwan) P. Sritara (Thailand) W.H. Van Gilst and J.W. Jukema (The Netherlands) O. Ergene (Turkey) A. Parkhomenko (Ukraine) A. Hall (UK) F. Kuster (Uruguay) N.V. Pham (Vietnam)
Mean follow-up of 2.75 years Study design A randomized, double-blind, placebo-controlled trial Ivabradine: starting dose of 7.5 mg bid, then 5, 7.5, 10 mg bid to reach target heart rate of 60 bpm Placebo run-in 2 - 4 weeks 19 102 patients randomized Matching placebo, bid M0 Inclusion M1 M48 or study end M6 M2 M3 Follow-up visit every 6 months Selection Fox K et al. Am Heart J. 2013;166(4):654-661.
Study end points Primary composite end point • Cardiovascular death • Nonfatal myocardial infarction Secondary end points • All-cause death • CV death • Coronary death • Nonfatal MI • Coronary revascularization • Elective coronary revascularization • New-onset or worsening heart failure Fox K et al. Am Heart J. 2013;166(4):654-661.
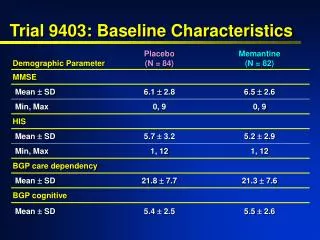
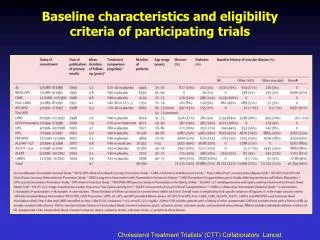
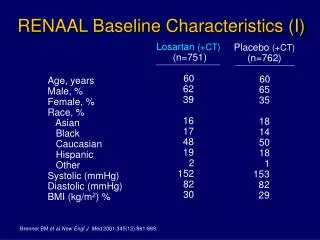
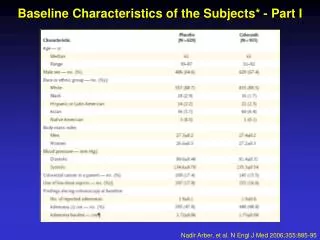
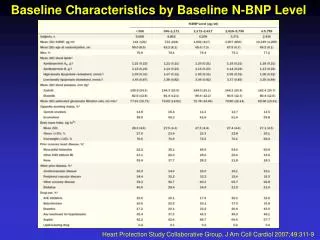
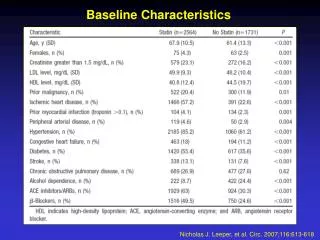
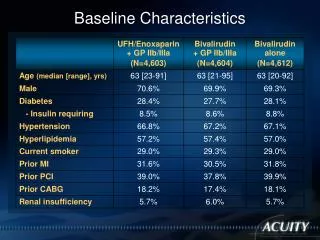
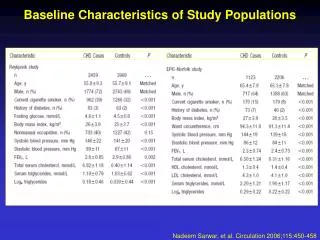
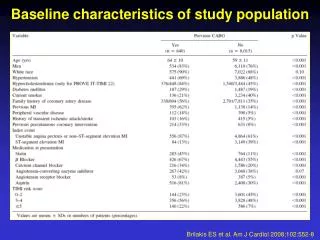
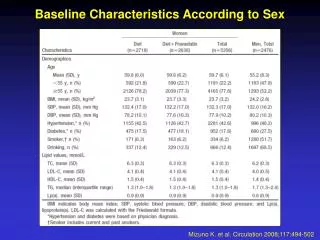
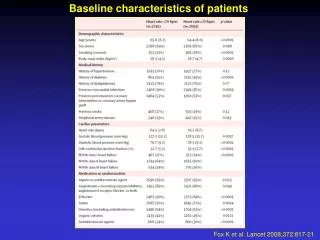
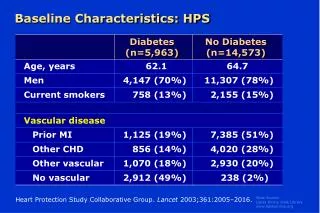
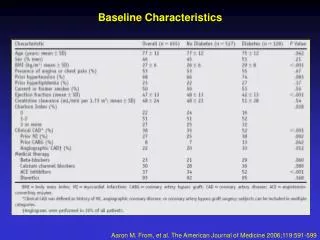
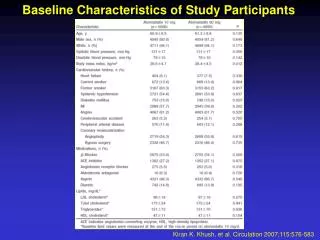
Baseline characteristics Fox K et al. Am Heart J. 2013;166(4):654-661.
Baseline characteristics Fox K et al. Am Heart J. 2013;166(4):654-661.
Background therapies Fox K et al. Am Heart J. 2013;166(4):654-661.
Use of background preventive therapies in clinical trials and registries
Substudies Fox K et al. Am Heart J. 2013;166(4):654-661.
Conclusion • Elevated resting heart rate is an important correlate of outcomes in patients with CAD • Heart rate lowering may therefore be expected to reduce mortality and cardiovascular event rates in patients with stable CAD • SIGNIFY will shed further light on the role of heart rate lowering with ivabradine in patients with stable CAD without clinical heart failure • The study is expected to end in 2014 Fox K et al. Am Heart J. 2013;166(4):654-661.