Download
1 / 141
1.42k likes | 1.67k Views
The Neuroscience of Orthopedics. Complex problems with simple solutions Roderick Henderson, PT, SCD, OCS, MA, CSCS. What You’ll Learn. Orthopedic diagnoses are often very straightforward The patient’s response to a diagnosis may vary according to: Sensory physiology

E N D
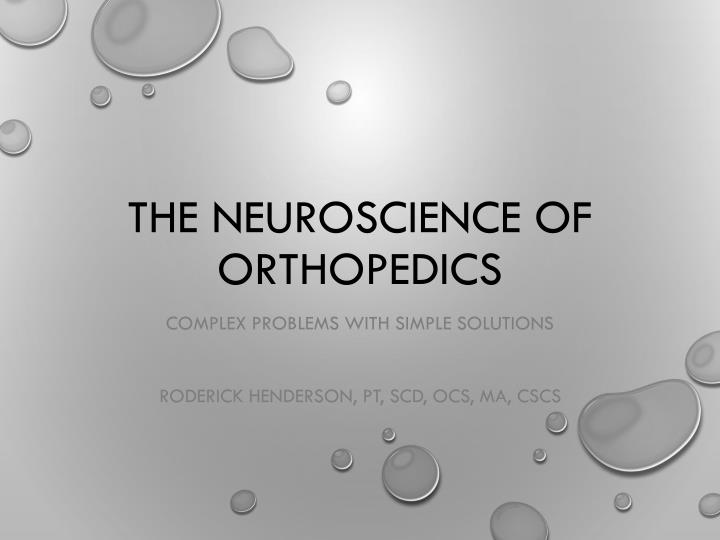
The Neuroscience of Orthopedics Complex problems with simple solutions Roderick Henderson, PT, SCD, OCS, MA, CSCS
What You’ll Learn • Orthopedic diagnoses are often very straightforward • The patient’s response to a diagnosis may vary according to: • Sensory physiology • Central processing (cognitive / affective) • Autonomic drive
The Nervous System • Drives the response • Adapts to new information
Where we’re going • How did we put the neuro in ortho? • How do we treat complex problems with straightforward solutions?
Orthopedic PT Stereotype • Formulaic • Protocol-driven • Boring…
What We Really See • Tremendous variability • Challenging problems • Exciting opportunities
Challenge #1 • Orthopedic PTs trained as clinical biomechanists • BUT – Lines between biomechanics and pathology are blurry!
Challenge #2 • We don’t like chasing pain • BUT - Pain is often the patient’s chief complaint!
Traditional Injury Model Symptoms Pathology Halderman S. Presidential Address, North American Spine Society: Failure of the pathology model to predict back pain. 1990; Spine 15:718-724.
Ideal Recovery Symptoms Pathology Halderman S. Presidential Address, North American Spine Society: Failure of the pathology model to predict back pain. 1990; Spine 15:718-724.
Expectations • Pathology and symptoms should improve with effective treatments • Ideally should also see a reversal of any structural abnormality
Persistent Pain Symptoms Pathology Halderman S. Presidential Address, North American Spine Society: Failure of the pathology model to predict back pain. 1990; Spine 15:718-724.
The Aging Body Symptoms Pathology Halderman S. Presidential Address, North American Spine Society: Failure of the pathology model to predict back pain. 1990; Spine 15:718-724.
A Growing Trend • Pathological signs present without symptoms (false positives) • Seen with increasing regularity • Lumbar spine • Shoulder • Foot and ankle
Consequences • Disability, fear, frustration • Higher costs, overutilization, dependence upon passive intervention
Still Bored?? • Thousands of new articles published • Evolving clinical guidelines • More ways to help our patients
Answers • Fully understanding response to injury • See where things go wrong • Treat the patient using a biopsychosocial model
Evolution of Pain Theory • Specificity • Gate • PainMatrix
Principles • Tissues have “pain” receptors • Pain signals transmitted to the brain
Key Assumptions • Pain is an input to the CNS • Pathology = Pain • Pineal gland is the pain center
Implications • Pathology = pain • Eradicate pathology = eradicate pain
Upside of Specificity • Upgrade from the mystical model! • Acknowledged the nervous system
Limitations of Specificity • Pain can be present without tissue damage • Tissue damage can be present without pain Key Note: Nociception is neither necessary nor sufficient for the production of pain
Other Problems • Phantom limb pain • Chronic regional pain syndrome Body parts are represented in the CNS through maps
Gate Theory (1965) • Descending control from brain and spinal cord • Formed the basis for TENS • Most PTs are aware of this model
What Changed? • Challenges the concept of “pain generator” • Noxious stimuli modulated by dorsal horn and CNS • Output is the “pain experience”
Limitations of the Gate • Widespread or chronic pain syndromes? • Pain following spinal cord injury • Still no accounting for CRPS! Melzack R. From the Gate to the Neuromatrix. Pain Supplement. 1999; 6:S121-S126.
Enter the Matrix • Also known as the “Pain Matrix” or “Neuromatrix” • Framework for multi-system response to injury • The most current model of injury response to date
Melzack R. Pain and the Neuromatrix in the Brain. Journal of Dental Education. 2001;65(12):1378-1382
Melzack R. Pain and the Neuromatrix in the Brain. Journal of Dental Education. 2001;65(12):1378-1382
What is an Input? • Brain constantly sampling information • Internal information from bodily tissues • External information from the environment
Inputs • Sensory • Cognitive • Affective
Butler D, Moseley P and DL. Explain Pain. 1st ed. Orthopedic Physical Therapy Products; 2003.
Relevance of Sensory Inputs • We are highly selective • Priority of inputs is variable • Altered by attention
Not a One-Way Street Butler D, Moseley P and DL. Explain Pain. 1st ed. Orthopedic Physical Therapy Products; 2003.
Clinical Relevance • Communication between tissue and CNS is bidirectional • Long-standing MSK problems show signs of neurogenic inflammation • Implications for neurodynamics
The Value of Good Input • Stimulus-detection system of the body • Tissue damage will increase signal intensity from that region • Purpose is to get your attention! • Sensory fibers are not purely sensory
Butler D, Moseley P and DL. Explain Pain. 1st ed. Orthopedic Physical Therapy Products; 2003.
Cognitive Inputs • Knowledge • Experience • Expectation
Cognitive Inputs • What does the patient believe is happening? • Have they dealt with similar problems?
Cognitive Inputs • How did they handle it? • What do they think is going to happen?
Relevance of Cognitive Inputs • Belief influence outcomes • Experience shapes coping • Expectation influences response
Affective Inputs • Baseline immune / endocrine function • Autonomic nervous system function • Limbic system – emotional regulation
Relevance of Affective Input • Interaction between nervous and immune • Autonomic function influences processing