Download
1 / 23
230 likes | 479 Views
Cases of the Month: December, 2008 . Clinicopathologic Exercises for Class of 2011 Paul Koles, MD, Director of Pathology Education Boonshoft SOM at Wright State University. Case 1: Headache in a 41-year-old woman.

E N D
Cases of the Month: December, 2008 Clinicopathologic Exercises for Class of 2011 Paul Koles, MD, Director of Pathology Education Boonshoft SOM at Wright State University
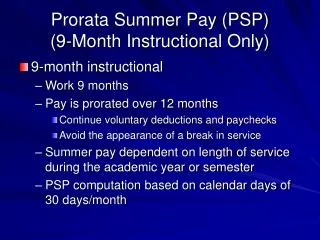
Case 1: Headache in a 41-year-old woman HISTORY: A 41-year-old woman had been in good health until one week earlier, when she developed a global headache, accompanied by generalized weakness, a sensation of imbalance, progressive anorexia, mild forgetfulness, and some blurring of vision. She came to the ambulatory clinic after these problems had persisted 7 days, where an imaging study revealed a brain mass. She was admitted to the hospital.
CT scan upon admission Horizontal (axial) CT scan of brain without contrast, at level of temporal lobes, showing increased density in the cortex of left temporal lobe, suggesting presence of hemorrhage (arrow). There is a surrounding area of low attenuation, representing edema of gray and white matter.
Past History • Native of El Salvador, immigrating to U.S. 11 years earlier. • Febrile illness 5 months before admission, with dyspnea, non-productive cough, and severe headaches that often woke her from sleep and improved when she sat up or stood. This illness had resolved quickly without treatment. • Married, 1 child (normal pregnancy and delivery) • No use of alcohol, tobacco, or birth control pills • Negatives: no history of previous neurologic or visual deficits, nausea, vomiting, seizures, chest pain, chills, sweats, melena, vaginal bleeding, weight loss. • HIV antibody test negative
Physical Exam • T 36.4C, P 72, R 18, BP 140/80 mm Hg • Alert, oriented, able to converse • Neck supple, no lymphadenopathy • Heart, lungs, abdomen, arms, legs normal • Neurologic exam: • All cranial nerve functions intact • Motor power 5/5 bilaterally; no pronator drift • Coordination normal • Deep tendon reflexes ++ arms & knees, + both Achillles • Plantar responses: flexor
Diagnostic Data on Admission • Urinalysis: 5-10 WBCs /high power field; a few bacteria /high power field • Erythrocyte sedimentation rate: 21 mm/hr (normal <20) • Hematocrit 35.8% (normal for adult female 37-47) • RBC mean corpuscular volume: 73 femtoliters (normal 78-100) • WBC count: 7,100 / microliter (61% neutrophils, 29% lymphocytes, 5% monocytes, 4% eosinophils, 1% basophils) • Platelet count 430,000 / microliter (normal 150,000 - 400,000) • prothrombin time 13.4 seconds (normal 11-14 seconds) • partial thromboplastin time 19.4 seconds (normal 20-35 seconds) • calcium 11.3 mg/dL (normal 8.9 - 10.7) • phosphorus 2.5 mg/dL (normal 2.4 - 4.5) • All other serum chemistries: normal (electrolytes, BUN, creatinine, glucose, uric acid, total bilirubin, magnesium, aspartate aminotransferase, creatine kinase, lactate dehydrogenase, alkaline phosphatase, thyroid stimulating hormone) • Chest radiograph: within normal limits • Electrocardiogram: normal rhythm, rate 74, no abnormalities
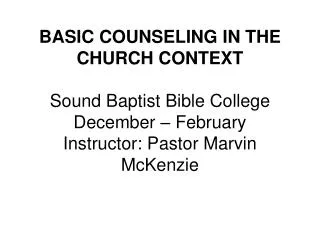
Additional Imaging Studies T1-weighted MR of brain obtained before contrast (A) and after contrast (B), showing hyperintense signal involving cortex of left temporal lobe, suggesting development of subacute stage of hemorrhage (methemoglobin). There is faint surrounding enhancement in panel B extending toward the ventricle, without evidence of subependymal spread. T2-weighted MR of brain at level of temporal lobes. Hyperintense signal suggests edema, and involves white matter more than gray matter
Hospital Course Treatment with phenytoin sodium, ranitidine, dexamethasone (4 mg every 6 hours), and vitamin K (10 mg orally for 3 days) was begun. She remained afebrile, with no changes on repeated neurologic exams. While she did not require urgent neurosurgical intervention for therapeutic benefit, it was decided to perform an open brain biopsy of the left temporal lobe for diagnostic purposes. This biopsy was performed under stereotactic imaging guidance (biopsy results are illustrated on next slide).
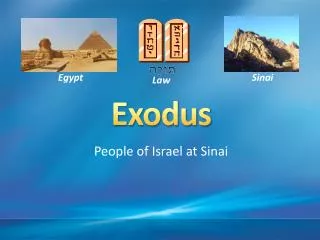
Histopathologic changes in stereotactic biopsy of left temporal lobe Leptomeninges, H&E 100x cerebral cortex, hematoxylin & eosin, 250x Leptomeninges, trichrome stain, 250x
Your Diagnosis? Case 1: The most likely diagnosis is • hemorrhagic infarction due to arterial embolus, resolving. • ischemic infarction due to arterial thrombus, resolving. c) necrotizing cerebral vasculitis (part of systemic vasculitis). d) subdural hematoma. • venous thrombosis with resolving infarction.
December 2008, Case 2: Progressive weakness in a 66-year-old man HISTORY: A 66-year-old right-handed man was admitted to the hospital because of progressive left-sided weakness. Two months before admission, he developed weakness of the left side of his face and left hand. A cranial MRI study was done (slide 3). During the three weeks before admission, the weakness worsened and his left leg also became weak. He denied fever, headaches, and visual problems. Past history includes a renal transplant from a living related donor 19 years ago for end-stage renal failure due to nephrolithiasis, alcoholic cirrhosis resulting in intermittent bleeding from esophageal varices and ascites, type 1 diabetes mellitus, coronary artery atherosclerosis, cholelithiasis, and osteoarthritis requiring bilateral hip replacements. He was a retired administrator. Smoked cigarettes for 15 pack-years, but quit 15 years ago. Long-standing ethanol abuse stopped 19 years ago. No illicit drug use. HIV antibody test was negative 10 years ago. Medications: NPH insulin, insulin lispro, azathioprine, prednisone, pantoprazole, vitamin B12, folic acid, vitamin B6, vitamin C, multivitamins, gabapentin, quetiapine, spironolactone, lactulose, and lorazepam.
(A) fluid-attenuated inversion recovery (FLAIR) image shows T2-weighted hyperintense lesion in posterior aspect of right frontal lobe involving white matter in a subcortical location, sparing the cortex, with no mass effect. (B) apparent-diffusion-coefficient map, the lesion (white oval) does not show restricted diffusion but shows hyperintensity that is more consistent with chronic changes than with acute infarction
Mental status and neurologic exam Normal mental status, fluent speech, mild dysarthria No neglect, correctly copied diagrams of clock and complex geometric shapes Cranial nerves: full visual fields with no extinction; left-sided facial droop with an upper motor neuron pattern. All other cranial nerve functions intact. Left arm and leg strength: deltoids, biceps, triceps 4/5; wrist extensors 3/5; wrist flexors 4/5; finger flexors 4/5; finger extensors 1/5; interossei 0/5, iliopsoas 4/5. Remainder of left leg muscles 5/5 Right arm and leg strength: 5/5 Sensation intact except left arm extinction of light touch on bilateral stimulation Deep tendon reflexes ++ bilaterally; ankle jerks absent. No clonus; left Babinski reflex present Cerebellar exam: normal finger-to-nose testing; gait limited by weakness of the left leg
A stereotactic brain biopsy was performed for diagnostic purposes. (see next slide)
Key to images: Four images from intraoperative smear preparation showing normal oligodendrocytes (arrowheads) and abnormal oligodendrocytes (arrows) in biopsy (H&E, 750X) B) Permanent section of biopsy, arrows on abnormal oligodendrocytes (H&E, 250x) C) Luxal fast blue stain for myelin (myelin stains dark blue) D) Immunohisto-chemical stain for neurofilament proteins in axons (axons stain brown)
Your diagnosis? Case 2: The most likely diagnosis is • Creutzfeldt-Jakob disease. • Encephalitis due to Herpes simplex. • Multiple lacunar infarctions. • Multiple sclerosis. • Progressive multifocal leukoencephalopathy.
Case 3: Dysphagia and weight loss in a 52-year-old woman HISTORY: A 52-year-old woman came to a physician’s office and told him, “I’m having trouble eating.” He asked, “Have you lost any weight?”, to which she replied, “About ten pounds over the last several months.” He then asked, “What kind of trouble are you having?”, to which she replied, “When I eat meat or salads, pieces of food seem to get stuck, and I have trouble swallowing them down.” He then asked, “Do you have any problem drinking liquids?”, to which she replied, “Usually not.” Several more questions, and a thorough review of systems, revealed 3 additional facts: her “trouble swallowing” had been occurring for the last 6 months. She stated “my hands get very cold” whenever she was outside on colder days, so she started wearing insulated gloves during the colder months, which seemed to help. She worked as a court reporter for the last 21 years, typing at a computer in the courtroom 4 - 7 hours per day Physical examination showed a normally developed, well-nourished female in no acute distress. Vital signs were within normal limits. The only abnormality identified was her hands (shown on next slide).
Case 3: physical exam Both hands (left); fingernail of left thumb (above)
Case 3: skin biopsy dermis The physician performed a punch biopsy of her skin from dorsum of right hand, between thumb and index finger, and sent the biopsy to pathology. Sections of the biopsy showed: subcutis Fascia deep to subcutis Epidermis and superficial dermis, H&E
Your Diagnosis? Case 3: The most likely diagnosis is Chronic dermatitis with fibrosis secondary to occupational-related injury. Cutaneous T-cell lymphoma. Rheumatoid arthritis. Scleroderma. Systemic lupus erythematosus.
Submit your answers by email • Submit your answers by email no later than midnight, January 5, 2009, to Ms. Ife Shafeek (ife.shafeek@wright.edu), administrative assistant for Dr. Koles, in this format: • Diagnoses for ______________ (fill in month) • Case 1: ______ (letter of your answer) • Case 2: ______ (letter of your answer) • Case 3: ______ (letter of your answer)