Download
1 / 39
390 likes | 543 Views
Adolescent Externalizing Behaviors. Joshua Leblang, Ed.S., LMHC Division of Public Behavioral Health and Justice Policy.

E N D
Adolescent Externalizing Behaviors Joshua Leblang, Ed.S., LMHC Division of Public Behavioral Health and Justice Policy
Our youth now love luxury. They have bad manners, contempt for authority, they show disrespect for their elders … they contradict their parents…and tyrannize their teachers." Socrates (c. 470-399 BC)
The number of boy burglars, boy robbers and boy murderers is so astoundingly large as to alarm all good men." New York Times editorial in 1857
Disruptive disorders, such as oppositional defiant disorder and conduct disorder, are characterized by antisocial behavior. It presents as collection of behaviors rather than a coherent pattern of mental dysfunction. As such, there is no “magic bullet” to fix the problem.
Normal Adolescent Development(AACAP, 2005) • Movement towards independence • More cohesive sense of identity • Ability to think ideas through • Conflict with parents begins to decrease • Increased ability for delayed gratification and compromise • Increased concern for others • Peer relationships important and take an appropriate place among other interests
Morals, Values, and Self-Direction • Greater capacity for setting goals • Interest in moral reasoning • Capacity to use insight • Increased emphasis on personal dignity and self-esteem • Social and cultural traditions regain some of their previous importance
For adolescents that you may encounter • It is rare that an adolescent self-refers themselves to counseling. • Externalizing youth are rarely interested in “insight” • Engagement with the youth is important, but equally important is parent/caregiver— • Ensure attendance at sessions. • Reinforcing any new behaviors • Provider of “reliable” information about behaviors.
Why do we need to know what works? • First, many programs, despite their good intentions, are either ineffective or actually do more harm than good. • Second, ineffective or harmful programs are a waste of scarce resources. Blueprints for Violence Prevention
Biases against Evidence-based Practices “They are too rigid and cookbook” “Doesn’t apply to real world kids with real world, multi-problem histories” “Developed in some lab” “Overly simplistic” “Too difficult to implement in community setting” “Just a band-aid and doesn’t address underlying issues and concerns” “Another passing fad” “My training and expertise are not valued”
Why use EBT’s Interventions showing beneficial effects in outcome research should be taught and used in preference to interventions that have not been tested and shown to be effective. • National Institute of Mental Health (National Advisory Mental Health Council Workgroup on Child and Adolescent Mental Health Intervention and Deployment, 2001), • Office of the Surgeon General (1999, 2004), • President’s New Freedom Commission on Mental Health (2003)
Rationale for Using Evidence-based Practices Programs that are integrative in nature (practice, research, theory) and use systematic clinical protocols ”clinical maps” Manual driven Model congruent assessment procedures Focus on adherence and treatment fidelity Clinically responsive and individualized to unique “outcome” needs of the client/family Models that have strong science/research support
Family Factors that Promote Resiliency(National Resilience Resource Center) Parent and family connectedness Parent/Adolescent activities Parental presence Parental school expectations Parents involvement and awareness of sexual behaviors Limit access to substances and weapons Seek help for parental and familial problems/concerns Seek support from other parents Know community resources
Program characteristics thatsupport positive youth development 1. Comprehensive, time-intensive 2. Earliest possible intervention 3. Timing is important 4. High structure is better 5. Fidelity to model is key to effectiveness
Positive Youth Development (con’t) 6. Need adult involvement 7. Active, skills-oriented programs are more effective 8. Programs that target multiple systems are most effective 9. Programs that are sensitive to the individual’s community and culture are best 10. Programs based on strong theoretical constructs and proven effective by evidence are best Connecticut Center for Effective Practice (From meta-analysis published in 2005)
3 Treatments top the list for adolescents ALL focus on family/ caregivers • Functional Family Therapy • Multidimensional Treatment Foster Care • Multisystemic Therapy
What is Functional Family Therapy? • Focus is to improve family communication and supportiveness while decreasing the intense negativity so often characteristic of these families. • Many of the targeted interventions, therefore, emphasize communication skills, family interaction, problem-solving and promoting constructive behaviors • Intervention ranges from, on average, 8 to 12 one-hour sessions up to 30 sessions of direct service for more difficult situations
What is Functional Family Therapy? • Conducted both in clinic settings as an outpatient therapy and as a home-based model • A treatment technique that is appealing because of its clear identification of specific phases, which organize intervention in a coherent manner, thereby allowing clinicians to maintain focus in the context of considerable family and individual disruption • Each phase includes specific goals, assessment foci, specific techniques of intervention, and therapist skills necessary for success
Multidimensional Treatment Foster Care (MTFC) Program Overview: The goal of the MTFC program is to decrease problem behavior and to increase developmentally appropriate normative and pro-social behavior in children and adolescents who are in need of out-of-home placement.
MTFC MTFC treatment goals are accomplished by providing: Close supervision; fair and consistent limits ; predictable consequences for rule breaking ; a supportive relationship with at least one mentoring adult; and reduced exposure to peers with similar problems. The intervention is multifaceted and occurs in multiple settings. The intervention components include: • Behavioral parent training and support for MTFC foster parents; • skills training for youth; • supportive therapy for youth; • school-based behavioral interventions and academic support; • and psychiatric consultation and medication management, when needed.
MULTISYSTEMIC THERAPY • Youths’ behaviors are influenced by their families, friends, and communities (and vice versa). • Families are the key to success, so all aspects of treatment are designed with full collaboration from the family. • Change can happen quickly, but it demands daily and weekly efforts from the youth and all the important people in his/her life. • Families can live successfully without involvement in social service agencies.
How is MST Different? • Discipline: Offers a combination of “best practice” treatments within a disciplined structure • Accountability: At all levels, providers are held accountable for outcomes through MST’s rigorous quality assurance system • Ecological validity: Working in the youth’s natural environment with existing family supports, thereby ensuring cultural sensitivity • Focus on long-term outcomes: Empowerment of caregivers to manage future difficulties; focus on sustainability
How Does MST “Work?” Intervention strategies: MST draws from research-based treatment techniques • Behavior therapy • Parent management training • Cognitive behavior therapy • Pragmatic family therapies • Structural Family Therapy • Strategic Family Therapy • Pharmacological interventions (e.g., for ADHD)
Why is MST Successful? • Treatment targets known causes of delinquency: family relations, peer relations, school performance, community factors • Treatment is family driven and occurs in the youths’ natural environment • Providers are accountable for outcomes • Staff are well trained and supported • Significant energies are devoted to developing positive interagency relations
Finding the Fit Positive & Strength Based Increasing Responsibility Present focused, Action-orientated Targeting Sequences Developmentally/ Culturally Appropriate Continuous Effort Evaluation & Accountability Generalization 9 Principles of MST
An ecological approach • Work with the entire ecology. By addressing the multiple systems, it is possible to make longer lasting changes for families. Community School Peers Family Youth Bronfenbrenner, 1979
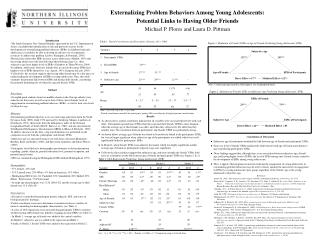
Condensed Longitudinal Model of Youth Antisocial Behavior Prior antisocial behavior Family Low Monitoring Low Affection High Conflict Antisocial Peers Antisocial behavior School Explaining delinquency and drug use, by D.S. Elliott, D. Huizinga and S.S. Ageton. Beverly Hills, CA: Sage Publications, 1985, 176 pp Low School Involvement Poor Academic Performance
Individual Factors • Antisocial behavior • Mental health problems • Low social conformity
FAMILY • Poor monitoring • Ineffective discipline • Low warmth • High conflict • Parental drug use/abuse
PEER • Association with drug-using peers, • Low association with prosocial peers
SCHOOL • Low achievement • Truancy • Low commitment to school
COMMUNITY FACTORS • High crime • Neighbors who use drugs • Transience
Meets other anti-social peers CYCLE CONTINUES No changes at home Returns home What usually happens to youth? Youth gets in trouble Sent to treatment
Meets other drug-using peers CYCLE CONTINUES What usually happens to youth? Sent to treatment / group Youth uses drugs Now has greater access to negative peers, people to buy from
Case Example • 16 year old male • Hx of truancy (missing school 2-3 days/week) • Runaway (usually 1-2 nights but as long as a week) • Defiant/oppositional –refuses to follow household rules
Case Example 2 • 14 year old female • Involved with negative peers • Reportedly gang-involved • Alcohol/marijuana usage • Stealing/shoplifting charges
House Bill 1373 • …up to twenty outpatient therapy hours per calendar year, including family therapy visits integral to a child's treatment How can we best use this???