Download
1 / 92
930 likes | 1.37k Views
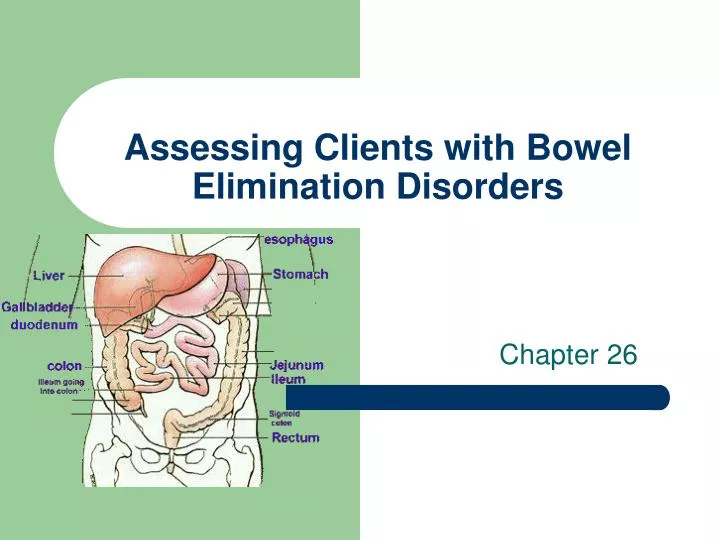
Assessing Clients with Bowel Elimination Disorders. Chapter 26. Review of Anatomy and Physiology. Small intestine pyloric sphincter to ileocecal junction three regions duodenum jejunum ileum Function - chemical digestion and absorption

E N D
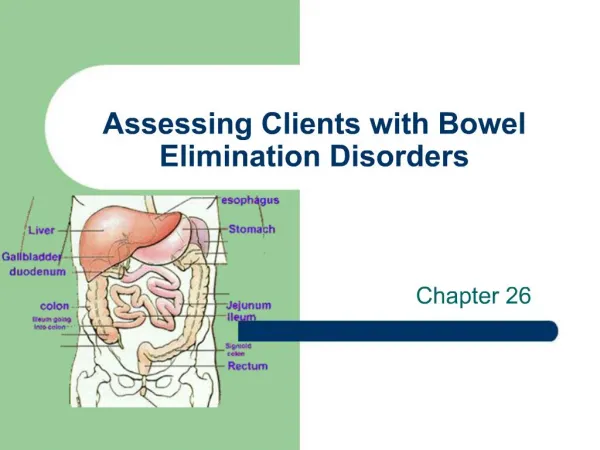
Assessing Clients with Bowel Elimination Disorders Chapter 26
Review of Anatomy and Physiology • Small intestine • pyloric sphincter to ileocecal junction • three regions • duodenum • jejunum • ileum • Function - chemical digestion and absorption • microvilli, villi and circular folds increase surface area
Review of Anatomy and Physiology • Large intestine - colon • ileocecal valve to anus • Cecum - first part of intestine - appendix • Colon divided into 3 parts • ascending • transverse • descending • Function - eliminate undigestible food, absorb water, salt and vitamins
Assessment of Bowel Function • Subjective • onset • characteristics • course • severity • precipitating factor • relieving factors • associated symptoms
Sample Interview Questions • Can you describe the type of cramping and abdominal pain you are having? • Have you every had bleeding from your rectum? • Have you noticed any changes in your bowel habits?
Assessing the Abdomen • Inspection, auscultation, percussion and palpation as described • Rectal exam - polyps • Stool for occult blood • + requires further testing for colon CA or GI bleeding 2nd to peptic ulcers, ulcerative colitis or diverticulosis
Blood and Stool • Melena - black tarry stool • Blood on Stool - bleeding sigmoid colon, rectum • Blood in Stool - colon, ulcerative colitis, • diverticulitis, tumor, ulcer • Stool black, hard = oral iron • Strong odor = blood of high fat content • steatorrhea
Nursing Care of Clients with Bowel Disorders Chapter 26
Disorders of Intestinal Motility • Diarrhea • serious in the young and elderly • increase in the frequency, volume and fluid content of the stool • Causes • bacteria, or parasitic infections, malaborption, medications, diseases, allergies or pyschological
Diarrhea • Clinical Manifestations • vary widely from several large watery stool to very frequent small stools • result in severe electrolyte imbalances • hypokalemia - Low K+ • hypomagnesemia - low Mg+ • hypovolemia - fluid volume deficit - hypovolemic shock with vascular collapse
Diarrhea • Collaborative Care • treat underlying cause • Labs • stool specimen - for WBC’s, parasitic infections culture • electrolytes - imbalance • Diagnostic tests • sigmoidoscopy - direct exam of bowel
Diarrhea • Client prep • consent, npo, enemas • Dietary management • fluid replacement - gatorade, pedialyte • bowel rest for 24 hours - add milk last • Pharmacology • absorbents, anticholinergics, antibiotics
The Client with Constipation • The infrequent or difficult passage of stool • two or less BM’s per week • affects elders - impaired health, medications, decrease physical activity • Diagnostics • Barium enema • - tumors, diverticular disease • colonoscopy • - tumor, obstruction, take bx
Constipation • Dietary Management • high fiber - vegetable fiber • adequate fluids • Pharmacology • laxatives for short term use • bulk form agents for long term use • enemas - acute short term or as prep
Irritable Bowel Syndrome • Disorder characterized by alternating periods of constipation and diarrhea • Cause - no organic cause found • related to food ingestion, meds., stress, hormones • looking at motor activity of the G.I. tract
IBS • Clinical Manifestations • Colic-like abdominal pain • Altered bowel elimination • mucous in stool, change in frequency, straining, urgency, incomplete emptying • Bloating, tenderness • Labs and Diagnostics • stool specimen, colonoscopy, UGI with SBFT • Dietary management • add fiber - adds bulk and water content
The Client with Fecal Incontinence • Loss of voluntary control of defecation • Causes • interfere with sensory or motor control of rectum and anal sphincters • neuro -spinal cord injury, head injury • local trauma - OB tears, anal-rectal injury, surgery • Other - radiation, impaction, tumors, confusion
Fecal Incontinence • Collaborative Care • dx made by history • digital exam - poor sphincter tone • treatment • bowel training program - establish regular pattern • dietary changes • stimulant - coffee, suppository, digital stimulation • surgery - colostomy
Acute Inflammatory and Infectious Disorders • Appendicitis • inflammation of the appendix • common cause of acute abd pain • most common reason for emergency abd surgery • most common in adolescents and young adults
Appendicitis • Simple • appendix is inflamed but intact • Gangrenous • tissue necrosis and microscopic perforations • Perforated • gross perforation and contamination of peritoneal cavity
Appendicitis • Clinical Manifestations • continuous mild generalized upper abd pain • then intensifies and localizes to RLQ • rebound tenderness - tenderness on release of pressure at McBurney’s point • + Rt heel tap pain • What about pain medications? • nausea, anorexia, vomiting, low-grade fever • perforation - increased pain, temp, abscess
Appendicitis Pathophysiology • The appendix can become obstructed by fecalith (hard masses of feces) a stone, inflammation or parasites. • As a result of the obstruction the appendix becomes distended with fluid. • This increases pressure within the appendix and impairs its blood supply. • The lack of blood supply leads to inflammation, edema, ulceration, and infection of the tissue. • Can become necrotic and perforate if treatment is not indicated.
Appendicitis • Interdisciplinary Care • Labs - CBC, UA, pregnancy test • Diagnostic studies - abd X-ray, pelvic exam, ABD ultrasound • Pharmacology - IV’s , antibiotics - third generation cephalosporin - rocephin • Surgery - Appendectomy - exploratory vs laproscopy
The Client with Peritonitis • Inflammation of the peritoneum - is the most significant complication of acute abdominal disorders • perforation of appendix, diverticulum, peptic ulcer, pancreatitis or GSW • bacterial infection - E coli or klebsiella
Peritonitis • Clinical Manifestations • Abdominal Effects • Diffuse or localized pain - rebound • Boardlike rigidity • diminished or absent bs • distention, anorexia, nausea, vomiting • Systemic effects • fever, malaise, tachycardia, restlessness • shock
Peritonitis • Labs and Diagnostics • CBC - WBC’s with shift to the left, immature wbc out to help fight infection • Blood culture - bacterial invasion into blood stream • Paracentesis - obtain peritoneal fluid • Abd x-ray - free air under diaphragm indicative of gastrointestinal perforation
Peritonitis - Interdisciplinary Care • Pharmacology • broad-spectrum antibiotics until culture report obtained • narcotic analgesic, antipyretics • Surgery - laparotomy • peritoneal lavage • washing out cavity with copious amounts of isotonic soln • drains - JP or pen rose, may be left open
Nursing Care - Peritonitis • NGT • intestinal decompression • Pain - abd distention and inflammation • assess - location, severity and type - analgesics • fowler’s - minimize stress on abd structures • alternative pain management - visualization, medication, relaxation
Nursing Care - Peritonitis • Fluid volume deficit • I & O, vs, wt., assess for dehydration • Altered protection • monitor for sign of infection, handwashing, aseptic technique for drsg changes • Anxiety • potential threat to life
The Client with Viral or Bacterial Infection • Gastroenteritis • describes general GI inflammation • syndrome - diarrhea, vomiting, anorexia, nausea and pain • organisms - Staphlococcal, Salmonella,Shigella, Botulism - life threatening, • Cholera - third world countries • dx - stool culture, tx - antibiotics, rehydration
Ulcerative Colitis • chronic inflammatory bowel disorder of the mucosa and sub mucosa . • Affects young 15-40 yrs old • Cause • unknown, genetic component, autoimmune, dietary factors - fiber poor foods, smoking • Affects the large bowel
Ulcerative Colitis • Clinical Manifestations • insidious onset - attack last 1 to 3 months • diarrhea - 30 to 40 stools per day with blood and mucus • fatigue, anorexia, generalized weakness • toxic megacolon - transverse colon is paralyzed may rupture, massive hemorrhage - need colostomy
Ulcerative Colitis • Interdisciplinary Care • supportive treatment • Dx - by sigmoidoscopy, edema, inflammation, mucus and pus • Pharmacology • Azulfidine - sulfonamide antibiotic, acts topically on colonic mucosa to inhibit inflammatory process • Dietary - npo with TPN, then low residue
Ulcerative Colitis • Surgery • not initial treatment • ileostomy • Nursing Care • relieving abd cramping • emotional support • teaching about illness and special needs • Nsg dx. - diarrhea and body image disturbance
The Client with Crohn’s Disease • Slowly progressive, relapsing inflammatory disorder of GI tract • diarrhea less severe, no blood or mucus • RLQ pain, fever, malaise, fatigue • affect young people 10-30 • can occur anywhere in the GI tract, patchy lesions
Crohn’s Disease • Interdisciplinary Care • therapy is directed toward managing the symptoms and controlling the disease process • Labs and Diagnostics • Stool specimen • X-ray - UGI with SBFT - shows ulcerations, strictures and fistulas • colonosocpy - bx
Crohn’s - Interdisciplinary Care • Pharmacology • same as ulcerative colitis - anti inflammatory • antidiarrheal - no risk of mega colon • Dietary • NPO - TPN, eliminate milk • Surgery • 2nd to complications, bowel obstruction - bowel resection