Download
1 / 75
760 likes | 995 Views
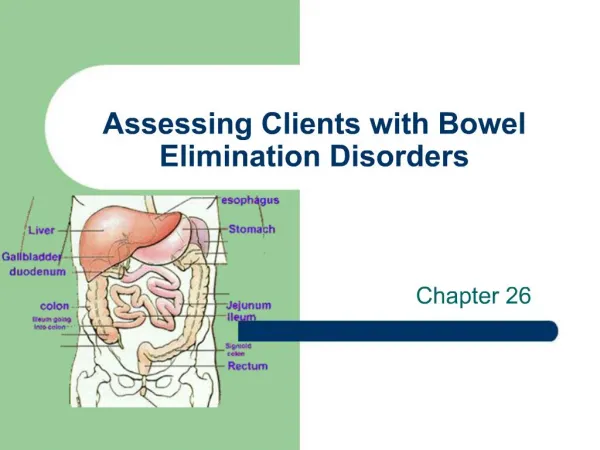
Bowel Disorders. Presnted by Shiva Golian , D.O. Disclosures. None. Objectives. Identify, diagnose and treat irritable bowel syndrome Identify, diagnose and treat fecal incontinence Identify, diagnose and treat pruritis ani. Irritable Bowel Syndrome.

E N D
Bowel Disorders Presnted by Shiva Golian, D.O.
Disclosures • None
Objectives • Identify, diagnose and treat irritable bowel syndrome • Identify, diagnose and treat fecal incontinence • Identify, diagnose and treat pruritisani
Irritable Bowel Syndrome • Syndrome: group of signs or symptoms that characterize a specific disorder • Type of functional GI disorder: chronic disorders of the GI tract in which an organic or structural lesion responsible for symptom development cannot be identified
IBSPrevalence and Epidemiology • Prevalence in North America: 10-15% • 2:1 female prevalence • Only 15% of those affected seek medical attention • Comprises 25-50% of all referrals to the gastroenterologist • After the common cold, second highest cause of work absenteeism • Peak prevalence: 3rdand 4th decades • Decreased prevalence in 6th and 7th decades • Dx should be made cautiously after age 60
IBSPathogenesis • Altered Gastrointestinal Motility • No predominant pattern: clustered contractions vs prolonged contractions • Exaggeration of the normal gut motility
IBSPathogenesis • Visceral Hypersensitivity • Distention • Balloon distention sensed at lower volumes • Rectal distention increased cerebral cortical activity • Bloating • Increased abdominal girth • Impaired transit of intestinal gas loads
IBSPathogenesis • Intestinal Inflammation • Some studies show an increased number of colonic lymphocytes, mast cells and plasma proinflammatory interleukins in those with IBS
IBSPathogenesis • Postinfectious • Associated with bacterial, protozoal, helminthic and viral infections • Thabane et al (meta-analysis of 18 studies) • Incidence of postinfectious IBS is 10% • Odds of developing IBS increase sixfold after acute GI infection • Risk factors: young age, prolonged fever, anxiety, depression • Causes of postinfectious bowel symptoms • Malabsorption: idiopathic bile acid malabsorption • Increase in enteroendocrine cells/lymphocytes: increased serotonin levels causes increased GI motility and visceral hypersensitivity • Antibiotic use
IBSPathogenesis • Change in the fecal microflora • Is there a role in probiotic use? Need more information
IBSPathogenesis • Small intestinal Bacterial Overgrowth (SIBO) • Pimental et al • 78% of 202 pts that met Rome I criteria for IBS had abnormal lactulose breath test suggestive of bacterial overgrowth • Very exciting news: this means that IBS can be cured with antibiotics • Unfortunately, more recent studies have failed to find any association between IBS and SIBO
IBSPathogenesis • Food Sensitivity • Food allergy: studies have been conflicting • Carbohydrate malabsorption: need more investigation • Gluten sensitivity: • Those without villous atrophy, presence of serum IgGantigliadin antibodies and expression of HLA-DQ2 may have a good response to gluten free diet • Make sure to confirm the absence of celiac disease
IBSPathogenesis • Genetics • Many studies with twins showing concordance rates ranging from 2-22% • One study found that having a parent with IBS was a greater independent predictor of IBS than having an affected twin • Thus it could be due to social learning • Genotyping studies • Perhaps an association with IBS and polymorphisms of serotonin transporter gene
IBSPathogenesis • Psychosocial Dysfunction • More lifetime and daily stressful events than control groups • Those with IBS have increased anxiety, depression, phobias and somatization • Positive association between IBS and abuse • Fukudo et al • Administration of corticotropin releasing factor (CRF – mediator of stress response) increases abdominal pain and colonic motility in IBS pts
IBS Diagnostic Criteria • Manning Criteria • Pain relieved with defecation • More frequent stools at the onset of pain • Looser stools at the onset of pain • Visible abdominal distention • Passage of mucus • Sensation of incomplete evacuation
IBS Diagnostic Criteria • Rome III criteria • Recurrent abdominal pain or discomfort at least 3 days per month in the last 3 months associated with 2 or more of the following: • Improvement with defecation • Onset associated with a change in frequency of stool • Onset associated with a change in form (appearance) of stool • Symptom onset at least 6 months prior to diagnosis • **Developed for clinical investigation; no emphasis on postprandial urgency, abdominal pain, diarrhea
IBSSubtypes • IBS with constipation (IBS-C): hard or lumpy stools >/= 25% or loose/watery stools <25% of BMs • IBS with diarrhea (IBS-D): loose or watery stools >/=25% or hard/lumpy stools <5% of BMs • Mixed IBS (IBS-M): hard/lumpy stools >/=25% or loose/watery stools >/=25% of BMs (most common group) • Unsubtyped IBS: insufficient abnormality of stool consistency to meet the above subtypes
DiagnosisHistory • 2 most common complaints • Abdominal pain • Required for diagnosis of IBS • Should be temporally related to defecation in some way • Location of pain varies from person to person, but is consistent over time in the individual • Altered bowel habits • But also remember bloating • Remember – these pts have an altered tolerance to normal amounts of distention
DiagnosisHistory • Be careful of alarm symptoms or “red flags” • Rectal bleeding • Nocturnal/progressive abdominal pain • Weight loss • Ask about travel history
DiagnosisPhysical • PE generally WNL • Abdominal exam • Tenderness – generally the LLQ • Should not have any rebound or guarding
Diagnosis • Good history and physical exam • Routine labwork (normal in IBS pts) • CBC • Chemistries • ESR • Stool samples for those with diarrhea • TSH for those with constipation • History with chronic symptoms, normal PE, normal labwork: accuracy of diagnosis is 95-97%
Diagnosis • Colonoscopy • Caucasians 50 or older • African Americans 45 or older • Strong family history of colorectal cancer or inflammatory bowel disease • Those with anemia • Those with stool WBCs • Those with alarm symptoms • Those with abnormal labwork • Diagnosis of exclusion
Treatment • No cure • Treatment focused on symptom relief • Must have a good therapeutic relationship • Kaptchuck et al • Pts with positive relationship with their healthcare provider have significantly more improvement • Patient education • Chronicity of syndrome • Normal life span
Treatment • Dietary • Efficacy of dietary modification not well established • Lactose • Exclusion of gas-producing foods • Food allergy testing: not well studied • Gluten sensitivity • Carbohydrate malabsorption: not enough large studies • Fiber: efficacy not proven
Treatment • Physical activity: potential benefit • Psychosocial therapies • May be beneficial in those with IBS symptoms associated with stressors • Benefits are controversial
Treatment • Pharmacotherapy • Antispasmodic agents • Dicyclomine (Bentyl) • Hyoscyamine (Levsin, Levbid, NuLev) • *Chlordiazepoxide/clidinium (Librax) • * Phenobarbital/hyoscyamine/atropine/scopolamine (Donnatal)
Treatment • Pharmacotherapy • Antidepressants • May be beneficial in those with neuropathic pain • TCAs have anticholinergic properties which help to slow intestinal transit time (helps with IBS-D) • Improvement in pain with TCAs occurs at lower doses than doses used for treatment of depression • TCAs to try: Amitriptyline (Elavil), imipramine (Tofranil), nortriptyline (Pamelor), desipramine (Norpramin) • Be careful with those with IBS-C • Other meds: paroxetine (Paxil), fluoxetine (Prozac), sertraline (Zoloft)
Treatment • Pharmacotherapy • Antidiarrheal agents • Loperamide (Imodium) – effective for tx of diarrhea, but not for tx of global IBS symptoms or abdominal pain • Alosetron (Lotronex) • 5-HT3 receptor antagonist • Used in females with IBS-D • Complications: ischemic colitis, severe constipation • FDA has brought this back under tight control
Treatment • Pharmacotherapy • Tegaserod (Zelnorm) • 5-HT4 receptor agonist • Used in IBS-C • Removed from market d/t cardiovascular side-effects • Lubiprostone (Amitiza) • Locally acting chloride channel activator • Best to use with for those with IBS with severe constipation where other approaches have failed • Used in IBS-C
Treatment • Pharmacotherapy • Linaclotide (Linzess) • Guanylatecyclaseagonist – stimulates intestinal fluid secretion and transit • Used for IBS-C • Antibiotics • Rifaximin – a nonabsorbable antibiotic • Improvement in bloating, abd pain, or altered bowel habits • Used in IBS without constipation • Benefits may be due to suppression of gas producing bacteria in colon
Treatment • Alternative therapy • Peppermint oil • Probiotics • Acupuncture • Enzyme supplementation • Hypnotherapy
Fecal IncontinenceBackground • In 1988 • Cost of adult diapers thought to exceed $400 million annually • Second leading cause of nursing home placement • Definition • Continuous/recurrent uncontrolled passage of feces (>10ml) for at least 1 month in someone > 3-4 yrs old
Fecal IncontinenceEpidemiology • Varies greatly depending on age, definition, setting: 1-24% • This may be an underestimation • Occurs in about 47% of nursing home residents
Fecal IncontinenceRisk Factors • Increasing age • Occurs in 15% of those >/= 70 • Poor general health • Physical limitations • COPD • IBS • Urinary incontinence • Chronic diarrhea • In women: depression and white race
Fecal Incontinence • Anatomic considerations
Fecal IncontinencePathophysiology • Dysfunction of anal sphincters • Abnormal rectal compliance • Decreased rectal sensation • Combination of the above
Fecal IncontinencePathophysiology • Dysfunction of anal sphincters • Vaginal delivery • Anal sphincter tears • Trauma to pudendal nerve: may cause incontinence years after delivery • Risks: • Forceps • High birth weight infant • Long second stage of labor • Occipitoposterior presentation of fetus
Fecal IncontinencePathophysiology • Dysfunction of anal sphincters • Surgical trauma • Anal fistula • Hemorrhoidectomy • After injection of botulinum toxin • Diabetes mellitus • Reduced internal anal sphincter resting pressure • Can be due to autonomic neuropathy
Fecal IncontinencePathophysiology • Decreased rectal compliance • Ability of rectum to store fecal debris is reduced • Leads to increased frequency and urgency • Leads to incontinence even if sphincter function is normal • Common conditions • Ulcerative colitis • Radiation proctitis
Fecal IncontinencePathophysiology • Impaired rectal sensation • DM • MS • Dementia • Meningomyelocele • Spinal cord injury
Fecal IncontinencePathophysiology • Fecal impaction • Elderly • Constant inhibition of internal anal sphincter • Overflow incontinence
Fecal Incontinence • History • Differentiate true incontinence from frequency and urgency • History of: • Prior vaginal delivery • Anorectal surgery • Pelvic irradiation • Diabetes • Neurologic disease • Do symptoms occur with a background of diarrhea?
Fecal Incontinence • Physical exam • Appropriate inspection of the perianal area • Fistula, prolapsing hemorrhoids, rectal prolapse • Anocutaneous reflex (anal wink sign) • Absence suggests nerve damage • Digital Rectal Exam • Mass, fecal impaction • Pt should be instructed to bear down and then squeeze against the finger
Fecal IncontinenceDiagnostic Procedures • Anorectalmanometry • Measures pressures • Decreased resting pressure suggests isolated IAS dysfunction • Decreased squeeze pressure suggests isolated EAS dysfunction
Fecal IncontinenceDiagnostic Procedures • Endorectal ultrasound/MRI • Good for identifying structural abnormalities of the anal sphincters, rectal wall, puborectalis muscle • Ultrasound much more economical • Findings correlate well with manometric findings
Fecal IncontinenceDiagnostic Procedures • Defecography • Barium paste is instilled into rectum • Pt is then seated on a radiolucent commode and films are taken at rest and during straining and defecation