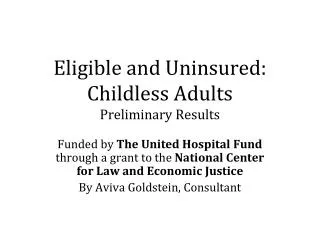
Download
1 / 14
140 likes | 287 Views
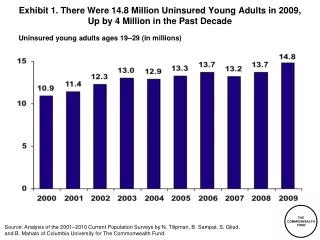
INTENSITY OF HEALTH SERVICES AND COSTS OF CARE FOR PREVIOUSLY UNINSURED MEDICARE BENEFICIARIES J. Michael McWilliams, M.D. Division of General Medicine Brigham and Women’s Hospital Department of Health Care Policy Harvard Medical School June 26, 2006. Uninsured Near-Elderly Adults.

E N D
INTENSITY OF HEALTH SERVICES AND COSTS OF CARE FOR PREVIOUSLY UNINSURED MEDICARE BENEFICIARIESJ. Michael McWilliams, M.D.Division of General MedicineBrigham and Women’s HospitalDepartment of Health Care PolicyHarvard Medical SchoolJune 26, 2006
Uninsured Near-Elderly Adults • ~4 million and growing (Baby Boom) • Difficulties acquiring coverage • Greater risk of declines than younger adults • Consequences of uninsurance more severe • Mortality: HR 1.43 uninsured vs. insured* • HR 1.56 among adults with chronic conditions • Proposals to expand coverage: Medicare buy-in *McWilliams, Zaslavsky, Meara, & Ayanian. Health Aff 2004
Study Rationale“The Committee hypothesizes that… uninsured persons gaining Medicare coverage at age 65 use health services more intensively and incur program costs higher than they would have had they been continuously insured prior to age 65… This question is one that merits further investigation.” -- Committee on the Consequences of Uninsurance, Institute of Medicine 2004
Health and Retirement Study (HRS) • 9,760 Adults ages 51-61 in 1992 • Biennial surveys through 2004 • Broad range of questions • Health insurance coverage • Physician visits in prior 2 years • Hospital admissions in prior 2 years • Medical expenditures in prior 2 years
Study Cohort:Near-Elderly with Chronic Conditions • Hypertension (HTN), Diabetes (DM), Heart Disease (CHD), or Stroke (CVA) • Excluded deaths and publicly insured • At least age 66 by 2004 • Insurance status prior to age 65: • Continuously Insured (all) n = 2090 • Ever Uninsured (1+y) n = 800 • Continuously Uninsured (3+y) n = 401
Statistical Analysis • Multiple waves before/after 65 (age 59 to 69) • Comparisons of utilization & expenditures: • Before and after Medicare coverage at age 65 • Differential increases • GLMs with log link function • GEEs to account for correlated data • Multiple Imputation for missing data • Propensity score weighting to adjust for observed characteristics at age 59-60
Hospital Stays: HTN, DM, CHD, CVAUnadjusted Differential Increase +0.15 (P<0.001) Δ <65 -0.01 (P=0.66) Δ >65 +0.14 (P<0.001)
Hospital Stays: HTN, DM, CHD, CVAAdjusted Differential Increase +0.15 (P=0.003) Δ <65 -0.04 (P=0.22) Δ >65 +0.11 (P=0.01)
Doctor Visits: HTN, DM, CHD, CVAAdjusted Differential Increase +2.6 (P<0.001) Δ >65 +1.8 (P=0.04) Δ <65 -0.8 (P=0.04)
Total Medical Costs: HTN, DM, CHD, CVAAdjusted Δ >65 +12,700 (P=0.10) Differential Increase+19,500 (P=0.005) Δ <65 -6,800 (P=0.008)
Conclusions • Significantly greater increases in health services and expenditures for previously uninsured adults gaining Medicare coverage • Uninsured near-elderly adults w/ chronic diseases required more intensive and costly care as Medicare beneficiaries than similar adults who were previously insured • Higher utilization after 65 exceeded lower utilization before 65
Policy Implications • Substantial downstream reductions in services and costs of care • Potential offsets to costs of coverage expansion • Total net costs of reform • Costs to Medicare • Importance of effective targeting • Subsidies for Medicare buy-in • Expand qualifying medical conditions