Download
1 / 1
10 likes | 229 Views
No. 218. Case series : Ruptured renal cysts presenting as solid l esions. Sliwinski, A. 1 , Kavanagh, L.E. 1 , Chan, Y. 1 , Lawrentschuk, N. 1 , Bolton, D. 1 , Clouston , D. 2 1 Department of Urology, Austin Hospital, Melbourne , Victoria , 2 Tissupath , Mount Waverley, Victoria.

E N D
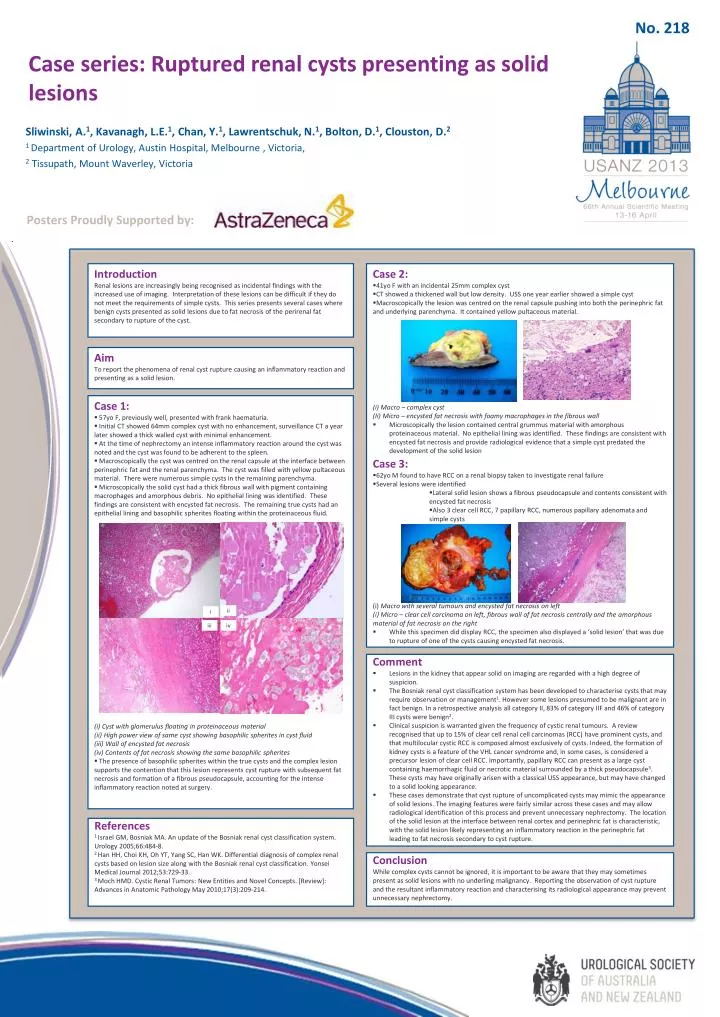
No. 218 Case series: Ruptured renal cysts presenting as solid lesions Sliwinski, A.1, Kavanagh, L.E.1, Chan, Y.1, Lawrentschuk, N.1, Bolton, D.1, Clouston, D.2 1 Department of Urology, Austin Hospital, Melbourne , Victoria, 2Tissupath, Mount Waverley, Victoria Posters Proudly Supported by: • Case 2: • 41yo F with an incidental 25mm complex cyst • CT showed a thickened wall but low density. USS one year earlier showed a simple cyst • Macroscopically the lesion was centred on the renal capsule pushing into both the perinephric fat and underlying parenchyma. It contained yellow pultaceous material. (i) Macro – complex cyst (Ii) Micro – encysted fat necrosis with foamy macrophages in the fibrous wall • Microscopically the lesion contained central grummus material with amorphous proteinaceous material. No epithelial lining was identified. These findings are consistent with encysted fat necrosis and provide radiological evidence that a simple cyst predated the development of the solid lesion • Case 3: • 62yo M found to have RCC on a renal biopsy taken to investigate renal failure • Several lesions were identified • Lateral solid lesion shows a fibrous pseudocapsule and contents consistent with encysted fat necrosis • Also 3 clear cell RCC, 7 papillary RCC, numerous papillary adenomata and simple cysts • (i)Macro with several tumours and encysted fat necrosis on left • Micro – clear cell carcinoma on left, fibrous wall of fat necrosis centrally and theamorphous material of fat necrosis on the right • While this specimen did display RCC, the specimen also displayed a ‘solid lesion’ that was due to rupture of one of the cysts causing encysted fat necrosis. Introduction Renal lesions are increasingly being recognised as incidental findings with the increased use of imaging. Interpretation of these lesions can be difficult if they do not meet the requirements of simple cysts. This series presents several cases where benign cysts presented as solid lesions due to fat necrosis of the perirenal fat secondary to rupture of the cyst. Aim To report the phenomena of renal cyst rupture causing an inflammatory reaction and presenting as a solid lesion. • Case 1: • 57yo F, previously well, presented with frank haematuria. • Initial CT showed 64mm complex cyst with no enhancement, surveillance CT a year later showed a thick walled cyst with minimal enhancement. • At the time of nephrectomy an intense inflammatory reaction around the cyst was noted and the cyst was found to be adherent to the spleen. • Macroscopically the cyst was centred on the renal capsule at the interface between perinephric fat and the renal parenchyma. The cyst was filled with yellow pultaceous material. There were numerous simple cysts in the remaining parenchyma. • Microscopically the solid cyst had a thick fibrous wall with pigment containing macrophages and amorphous debris. No epithelial lining was identified. These findings are consistent with encysted fat necrosis. The remaining true cysts had an epithelial lining and basophilic spherites floating within the proteinaceous fluid. (i) Cyst with glomerulus floating in proteinaceous material (ii) High power view of same cyst showing basophilic spherites in cyst fluid (iii) Wall of encysted fat necrosis (iv) Contents of fat necrosis showing the same basophilic spherites • The presence of basophilic spherites within the true cysts and the complex lesion supports the contention that this lesion represents cyst rupture with subsequent fat necrosis and formation of a fibrous pseudocapsule, accounting for the intense inflammatory reaction noted at surgery. ii i iii iv • Comment • Lesions in the kidney that appear solid on imaging are regarded with a high degree of suspicion. • The Bosniak renal cyst classification system has been developed to characterise cysts that may require observation or management1. However some lesions presumed to be malignant are in fact benign. In a retrospective analysis all category II, 83% of category IIF and 46% of category III cysts were benign2. • Clinical suspicion is warranted given the frequency of cystic renal tumours. A review recognised that up to 15% of clear cell renal cell carcinomas (RCC) have prominent cysts, and that multilocular cystic RCC is composed almost exclusively of cysts. Indeed, the formation of kidney cysts is a feature of the VHL cancer syndrome and, in some cases, is considered a precursor lesion of clear cell RCC. Importantly, papillary RCC can present as a large cyst containing haemorrhagic fluid or necrotic material surrounded by a thick pseudocapsule3. These cysts may have originally arisen with a classical USS appearance, but may have changed to a solid looking appearance. • These cases demonstrate that cyst rupture of uncomplicated cysts may mimic the appearance of solid lesions. The imaging features were fairly similar across these cases and may allow radiological identification of this process and prevent unnecessary nephrectomy. The location of the solid lesion at the interface between renal cortex and perinephric fat is characteristic, with the solid lesion likely representing an inflammatory reaction in the perinephric fat leading to fat necrosis secondary to cyst rupture. References 1Israel GM, Bosniak MA. An update of the Bosniak renal cyst classification system. Urology 2005;66:484-8. 2 Han HH, Choi KH, Oh YT, Yang SC, Han WK. Differential diagnosis of complex renal cysts based on lesion size along with the Bosniak renal cyst classification. Yonsei Medical Journal 2012;53:729-33. 3 Moch HMD. Cystic Renal Tumors: New Entities and Novel Concepts. [Review]: Advances in Anatomic Pathology May 2010;17(3):209-214. Conclusion While complex cysts cannot be ignored, it is important to be aware that they may sometimes present as solid lesions with no underling malignancy. Reporting the observation of cyst rupture and the resultant inflammatory reaction and characterising its radiological appearance may prevent unnecessary nephrectomy.