Download
1 / 41
410 likes | 659 Views
Renal Cell Carcinoma & Other Solid renal lesions. Dr Charles Chabert POW May 2005. Epidemiology. 12 th most common site in men /17 th female Low amongst Asian & African Highest in Czech Republic: 20/10 per 100,000. WHO 2004. Epidemiology. Increase in all groups till mid ’80s

E N D
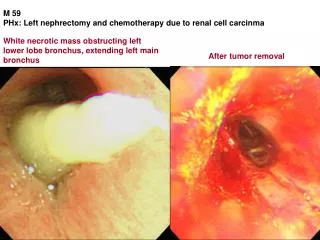
Renal Cell Carcinoma & Other Solid renal lesions Dr Charles Chabert POW May 2005
Epidemiology • 12th most common site in men /17th female • Low amongst Asian & African • Highest in Czech Republic: 20/10 per 100,000 WHO 2004
Epidemiology • Increase in all groups till mid ’80s • Increase in incidence after age 40 years • Decrease after age 75 years • Male more commonly affected WHO 2004
Aetiology Environmental • Tobacco smoking • Carcinogenic arsenic • Asbestos, cadmium, organic solvents, fungal toxins • Body Mass Index • Hypertension • Phenacetin WHO 2004
Genetic Basis For RCC • von Hippel-Lindau (VHL) • Birt-Hog-Dube (BHD) • Hereditary Papillary renal CA • Hereditary Leiomyomatosis & RCC Syndrome Pavlovich et at Urol Clin N Am 30,2003 437-454
von Hippel-Lindau • First described by opthalmologists • Autosomal dominant inherited • VHL gene located at 3p25 • pVHL = Tumour suppressor gene Pavlovich et at Urol Clin N Am 30,2003 437-454
von Hippel-Lindau Manifestations • Renal cysts, Clear cell RCC • Haemangiomas of retina & CNS • Phaeochromocytoma • Pancreatic cysts • Endolymphatic sac • Epididymal papillary cystadenomas Pavlovich et at Urol Clin N Am 30,2003 437-454
von Hippel-Lindau Type 1 No phaeochromocytoma Type2a Phaeochromocytoma CNS & Retina haemangioblastomas Type2b + pancreatic involvement Pavlovich et at Urol Clin N Am 30,2003 437-454
Clinical Features • Retinal lesions occur first • Mean onset 25 years • CNS haemangiomas later- 30years • Renal lesions – 37 years
Clinical Diagnosis • Haemangioblastoma of CNS or retina & extraneuronal lesion • + Family History • Any one lesion Pavlovich et at Urol Clin N Am 30,2003 437-454
Birt-Hog-Dube • Autosomal dominant • Fibrofolliculomas • Pulmonary cysts (90%) • Spontaneous pneumothorax (20%) • Renal neoplasms (25%)– hybrid oncocytic RCC Pavlovich: J Urol, 173(5). May 2005 1482-1486
Hereditary Papillary RC • Autosomal dominant - 50% penetrance • Papillary RCC • Late onset, bilateral & multiple • Gene location 7q31 - mutations MET
Hereditary Papillary RC • MET: proto-oncogene • Induces mitogenesis, morphogenesis and cellular migration • No documented extrarenal manifestations
Hereditary Leiomyomatosis & RCC • Aggressive PRCC • Uterine leiomyomas/ leiomyosarcomas/ cutaneous nodules • Single lesions & early metastasis
Clinical Features of RCC • Classic triad • Incidental finding • Systemic symptoms • Paraneoplastic syndromes – 30%
Paraneoplastic Syndromes • Haematological: • Anaemia • Raised ESR • Stauffer syndrome • Fever
Paraneoplastic Syndromes • Amyloidosis: 8% • Hypercalcaemia: 5-13% • Erythrocytosis: 3-10% • Hypertension: 10-40%
Histologic Subtype • Clear cell RCC: 70% • Multilocular RCC Reduced mets & LR • Papillary: 15% less aggressive 2 subtypes; type 2 more aggressive Leibovich et al Uro Clin Am 30 (2003) 481-497
Histology • Chromophobe RCC: 5% Excellent prognosis Mets rare- propensity for liver • Collecting Duct RCC: <1% Aggressive Rapid mets Leibovich et al Uro Clin Am 30 (2003) 481-497
Grading • Fuhrman System: 4 grades • Features assessed: • Nuclear size, contour, nucleoli • Grade 1: 86% 5 yr survival • Grade 4: 24% 5yr survival
Staging • AJCC TNM 2002 • Changes from 1987-1997:stage T1 cutoff • 2002: T1 substratified into T1a & T1b • Validated by Salama et al: J Urol 173(5) May 2005.1492-1495
Management • Radical nephrectomy • Does Lap nephrectomy reproduce open technique? • Issues: • Early vascular control • LN dissection • Adrenal gland
Lymph Node Dissection • LN dissection unnecessary, if node –ve on imaging • No difference in 5yr survival. • 2% node positive – correlates with EORTC 1% Minervini et al BJU Int 2001;88:169-72
Adrenelectomy • Large upper pole tumour or involved on CT • Overall Incidence 5.7% • T1-2 0.6% • T4 40% Tsui et al J Urol 2000:163;437-41
Oncological Outcome • 5 year recurrence free & CA specific survival 92% & 98% Portis et al J Urol 2002;167:1257-62
Conclusion • Laparoscopic approach mirrors open • New gold standard
Other Solid lesions • Oncocytoma • Aniomyolipoma • Adenoma
Oncocytoma • Benign epithelial neoplasms • Mitochondria-rich, eosinophilic cytoplasm • 5% renal neoplasms • Centrally placed scar, spoke-wheel pattern
Angiomyolipoma • Benign mesenchymal tumour • Adipose tissue, smooth muscle & abnormally thickened blood vessels • Independently or in association with TS
Metanephric Adenoma • Rare condition recently diagnosed • Benign course • Histopathological diagnosis
Conclusion • AML can be distinguished radiologically • Others managed accordingly