Download
1 / 65
760 likes | 1.98k Views
The Shoulder Complex. Its mobility compromises stability. Structurally, the shoulder is an unstable joint relies on a large network of ligaments and muscles to provide stability without restricting mobility. Functional movement involves integration of bones, joints, ligaments, and muscles.

E N D
The Shoulder Complex • Its mobility compromises stability. • Structurally, the shoulder is an unstable joint • relies on a large network of ligaments and muscles to provide stability without restricting mobility. • Functional movement involves integration of bones, joints, ligaments, and muscles.
Glenohumeral Flexion Extension Abduction Adduction Internal Rotation External Rotation Shoulder Girdle Protraction Retraction Elevation Depression Upward Rotation Downward Rotation Shoulder Motion
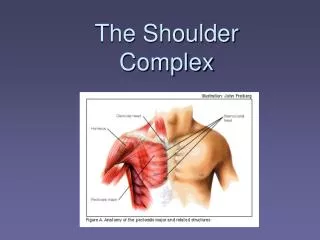
Functional Anatomy • Bones • Humerus • Angle of inclination • 130-150o • Angle of torsion • Varies • Scapula • Clavicle
Functional Anatomy • Four Joint System • Glenohumeral Joint • Scapulothoracic Joint • Acromioclavicular Joint • Sternoclavicular Joint Rhythm between the joints
Functional Anatomy • Glenohumeral joint • Ball and socket – • glenoid fossa is 2/3 size of the humeral head. • Static stabilizers • What are these? • Dynamic stabilizers • What are these?
Glenohumeral Ligaments Circle Stability The anterior, inferior, superior, and posterior glenohumeral ligaments act together to force the articular surface of the humeral head against the glenoid. As one is stretched the other develops tension. Static Stabilizers
Glenoid labrum Cartilage Thicker on outside and thinner on inside Circle stability Acts like tee for a golf ball Complimented by ligaments and long head of biceps tendon Static Stabilizers
Coracoacromial Arch Coracoacromial Ligament Roof Supraspinatus Long head of Biceps Tendon Superior/Anterior Labrum Bursa = Subacromial (aka Subdeltoid) Functional Anatomy
Dynamic Stabilizers • Glenohumeral dynamic stabilizers • Originate on axial skeleton and attach to humerus • Latissimus dorsi, serratus anterior, pectoralis minor, and pectoralis major • Originates on scapula/clavicle and attach to humerus • Deltoid, teres major, coracobrachialis, biceps and triceps. • Rotator Cuff - SITS
Rotator cuff Supraspinatus Infraspinatus Teres Minor Subscapularis Shoulder Musculature What is the function of the rotator cuff?
Force couples - Circle stability Co-contraction – compresses the humeral head within the glenoid fossa = minimizes humeral head displacement Adducted position – rotator cuff vs. anterior deltoid Abducted position – rotator cuff and long head of biceps vs. deltoids Dynamic Stabilizers
Functional Anatomy • Scapulothoracic joint – not a true joint • Upward rotation, downward rotation, protraction, and retraction • When do these occur in throwing motion? • It is essential to maintain positioning of humeral head relative to glenoid and for glenoid to adjust relative to movement while maintaining stable base. • Scapulohumeral Rhythm • Is often the key to shoulder pathology • 180 degrees of motion – flexion or abduction • 120o Glenohumeral • 60o Scapulothoracic – Upward rotation/Tilt
Scapulohumeral Rhythm • Humeral to Scapular ratio ( • Humeral Elevation to Upward Rotation
Dynamic stabilizers Trapezius, levator scapulae, pectoralis minor, serratus anterior, and major and minor rhomboids. Which are upward and which are downward rotators? Which are protractors and retractors? Serratus anterior Very important especially deceleration/follow-through of throwing Scapular Stabilizers
Functional Anatomy • Sternoclavicular joint • Must have motion here to achieve full humeral abduction • Interclavicular, Sternoclavicular ligaments • Acromioclavicular joint • Must have posterior rotation of clavicle so scapula can rotate to allow full elevation. • Trapezoid and Conoid ligaments
Kinetic Chain • Interaction of the sternoclavicular, acromioclavicular, scapulothoracic, and glenohumeral joints. • To get overhead motion: • Scapula must rotate. • Clavicle elevates.
Mechanisms of Injury • Direct Trauma
Mechanisms of Injury • Indirect Trauma
Winging Scapula Mechanisms of Injury • Shoulder Dyskinesis
Sternoclavicular Injuries • MOI: • Direct contact • Transfer through kinetic chain – longitudinal force through clavicle – FOOSH or Traction • Grades 1, 2, 3 - (sprain to dislocation) • Painful motions – Retraction, Protraction, Elevation • Dislocation • Anterior more common. • Posterior is very serious – Why? • S/S: Dizziness, nausea, neurovascular changes, or dysphagia • Testing – Joint play and palpation • Tx: • Ice, Sling, and Referral • Figure 8 immobilization – 3-5 weeks • Rehabilitation
Ligaments: Acromioclavicular ligament Coracoclavicular ligaments – Trapezoid and Conoid MOI: Direct trauma FOOSH or tip of elbow Top of shoulder Clavicle Chronic degeneration - overuse Classification Type I, II, III, IV, V, VI Step-off deformity S/S: PAIN, laxity, deformity Radiating pain – neck/scapula Acromioclavicular Injuries
Special tests: AC Glide -Piano Key Sign Pain above 90o and with horizontal adduction Traction, Compression Tx: Conservative – 1-4 weeks Ice, sling, corticosteroid injections, leukotape Rehabilitation/Padding Surgical – at least 4 months Resection of distal clavicle Wires for stability Acromioclavicular Injuries
Shoulder Instability vs. Laxity • Is there a difference? • Descriptions • Laxity – Capsular weakening and stretching that allows humeral head to have large glide motion in one or more directions • Puts many structures at risk by demanding more effort to control motion. • Instability – Humeral head displacement with elevation • Many causes – laxity, weakness, neurological
Glenohumeral Sprain • Damage to capsular ligaments • MOI: • forceful movement – abduction and rotation • S/S: • Pain/tenderness • Limited ROM – end ranges • Laxity tests • Apprehension • Glenohumeral Glide • Potential for chronic problems • Importance of immobilization and strengthening
Glenohumeral Dislocations • Dislocations and Subluxations • What’s the difference? • MOI: Dislocation • Direct trauma (laxity) - FOOSH • 85-90% will reoccur if MOI was direct trauma • Indirect trauma (instability) • General S/S: • Joint dislocation – not functioning • Pain • Vascular or Neurological problems? • When do athletes need surgery? • What are complications?
Glenohumeral Dislocations • Classification • Anterior Glenohumeral - most common • MOIs • Bankart lesion and Hills-Sachs lesion • Posterior Glenohumeral • MOIs • Reverse Hills-Sachs lesion • Inferior Glenohumeral - very uncommon • MOIs
Glenohumeral Dislocations • S/S: • classic deformities for each direction • Special Tests: • Glide tests, Apprehension, Load and Shift, Relocation, and Sulcus Sign • Clunk (R/O Labral Tear) • Tx: No surgery • Who reduces? • Ice/Modalities • Immobilization – 3-4 weeks • Strengthening • Rotator cuff and scapular
Chronic Shoulder Subluxation • MOI: Traumatic, Atraumatic, or Microtraumatic • Types: • Anterior – • clicking or pain; complain of dead arm during cocking phase (when throwing); pain posteriorly; possible impingement; positive apprehension test • Posterior – • possible impingement, loss of internal rotation; crepitation; increased laxity; pain anteriorly and posteriorly • Multidirectional (MDI)– • inferior laxity; positive sulcus sign; pain and clicking w/ arm at side; possible signs and symptoms associated w/ anterior and posterior instability
Chronic Shoulder Subluxation • Tests: Clunk and O’Brien’s • S.L.A.P. lesions = complication • Superior labrum anterior to posterior • Long Head of Biceps Brachii • Types I, II, III, IV
Chronic Shoulder Instability or Laxity • Management • Conservative • strengthening (rotator cuff and scapula stabilizers) • Various harnesses and restraints can be used to limit motion • Surgical stabilization may be required to improve function and comfort • Usually not chosen unless had two traumatic dislocations ornon-traumatic dislocations • 6 to 8 weeks immobilization
Shoulder Injuries • Fractures of the Humerus • Shaft or Proximal fracture • MOI: Direct blow or FOOSH • Epiphyseal fractures • MOI: Direct blow or indirect loading • common in young athletes • May pose danger to nerve and blood supply
Shoulder Injuries • Fractures of the Humerus • Signs and Symptoms • Pain, swelling, point tenderness, decreased ROM • Management • Immediate application of splint, treat for shock and refer • Humeral fractures- remove from activity for 3-4 months • Proximal fracture - incapacitation 2-6 months • Epiphyseal fracture - quick healing - 3 weeks <>
Shoulder Injuries • Contusion of Upper Arm • Etiology • Direct blow • Signs and Symptoms • Transitory paralysis and inability to use extensor muscles of forearm • Ecchymosis • Management • RICE for at least 24 hours • Provide protection to contused area to prevent repeated episodes that could cause myositis ossificans • Maintain ROM
Shoulder Injuries • Clavicular Fractures • MOIs: • FOOSH, fall on tip of shoulder or direct impact • Occur primarily in middle third (greenstick fracture often occurs in young athletes) • Signs and Symptoms • Supporting of arm, head tilted towards injured side w/ chin turned away • Clavicle may appear lower • Pain, swelling, deformity and point tenderness • Management • Closed reduction - sling and swathe, immobilize w/ figure 8 brace for 6-8 weeks • Rehabilitation and use of a sling for 2-4 weeks
Biceps Rupture MOI: Result of a powerful contraction Generally occurs near origin of muscle at bicipital groove Signs and Symptoms “Snap” and intense pain Protruding bulge– “popeye” Definite weakness with elbow flexion and supination Management Ice, Sling, and refer Athletes will require surgery Older individual will be able to rely on brachialis which serves as primary elbow flexor Shoulder Injuries
Shoulder Injuries • Repetitive Throwing or Overhead Motion Injuries • Rotator Cuff Pathology • Rotator Cuff Impingement Syndrome • Compressive vs. Tensile • Rotator Cuff Tendinitis • Overhead Athlete and Instability Continuum • Instability = unwanted humeral translation as a result of ineffective muscle contraction
Overhead Athlete and Instability Continuum Overuse Microtrauma = Inflammation Instability Subluxation Impingement Rotator Cuff Tendinitis Rotator Cuff TEAR Pink and Jobe, 1991
MOI Mechanical compression of supraspinatus tendon, subacromial bursa and long head of biceps tendon due to decreased space under coracoacromial arch Seen in over head repetitive activities Exacerbating factors - laxity and inflammation, postural mal-alignments Rotator Cuff Impingement
Primary compression Irregularly shaped acromion or ligament, enlarged bursa, inflammed tendons Secondary compression Instability, poor posture, repetitive overhead Primary tensile Overuse, Posterior capsule tightness, and rotator cuff weakness Secondary tensile Scapular dyskinesis, rotator cuff weakness, instability Impingement Inflammation Rotator Cuff Impingement
Rotator Cuff Impingement • Signs and Symptoms • Diffuse pain, pain on palpation of subacromial space, bicipital groove, supraspinatus insertion • Limited ROM – active and passive – above 90o • Painful arc – 70-120o • Decreased strength of external rotators compared to internal rotators; tightness in posterior and inferior capsule • Special Tests: Neer’s and Hawkins-Kennedy Tests. Empty Can • Tx: Rehabilitation – rotator cuff and scapular stabilizers
Rotator Cuff Tendinitis • Supraspinatus most likely • Etiology either Insidious or Acute • MOI: Overuse; Instability; Impingement; acromion spurs; poor vascularization (“wringing out”) • 3 Stages - I - inflammation; II - degeneration; III – tear • S/S: pain deep in shoulder and radiating down lateral arm; pain w/ follow –through or overhead, supraspinatus tenderness, decreased strength – abd, ER, IR • Special tests – Empty Can and Drop test; Impingement tests
Stage I – Supraspinatus or biceps tendon injury Pain w/ abduction and resisted supination w/ external rotation; Edema and thickening of rotator cuff and bursa Occurs in athlete < 25 years old Stage II – Permanent thickening and fibrosis of supraspinatus and biceps tendon; pain w/ motion Aching during activity that worsens at night Stage III – History of shoulder problems and pain Limited active and full passive ROM Tendon defect (3/8 “) or tear – partial thickness tear Permanent scar tissue and thickening of rotator cuff Athletes 25-40 years old Stage IV- Infraspinatus and supraspinatus wasting Pain during abduction and ER Tendon defect greater than 3/8” – full thickness tear Limited active and full passive ROM Rotator Cuff Pathology