Download
1 / 22
230 likes | 342 Views
Three days vs five days oral cotrimoxazole therapy in non-severe pneumonia. Samir K. Saha and Cotrimoxazole Study Group Indonesia and Bangladesh. Back ground. WHO recommendation for Non-Severe pneumonia. Cotrimoxazole or Amoxicillin for 5 days Attention to shorter course of therapy

E N D
Three days vs five days oral cotrimoxazole therapy in non-severe pneumonia Samir K. Saha and Cotrimoxazole Study Group Indonesia and Bangladesh.
Back ground • WHO recommendation for Non-Severe pneumonia. • Cotrimoxazole or Amoxicillin for 5 days • Attention to shorter course of therapy • Better understanding about the role of antibiotic • ICDDR,B experience with drop-outs • Pakistan experience with Short course amoxicillin therapy. • Implications on Compliance, Cost and Microbial resistance.
Aims • To determine the equivalence of 3 and 5 days of oral Cotrimoxazole for the treatment of non severe pneumonia. • To study the impact of cotrimoxazole treatment on carriage strains of Streptococcus pneumoniae and Haemophilus influenzae.
Study design • Double blind, Randomized, Placebo-controlled equivalence trial. • Study was conducted from July 2001 to May 2003. • Ethical clearance was obtained from the ERC of Bangladesh Institute of Child Health and Hasan Sadikin General Hospital.
Sample Size Calculation • Sample size was calculated to compare the clinical failure and/or success in two treatment groups. • Expecting 12% treatment failure rate in 5 days group. • Based on previous finding of 9-13% failure • With a sample size of 887 in each group calculated to give 90% power to reject the null hypothesis: 3 day and 5-day treatment are not equal.
Inclusion criteria Age 2-59 months WHO defined non-severe pneumonia with or without wheezing. Consent given Exclusion criteria Having severe pneumonia or other very severe disease Allergic to cotrimoxazole Acute Asthma Prior enrollment in the study. Required antibiotic for any other disease(s) Previous hospitalization in last two weeks. Prior antibiotic Weight <4.0 kg Screening of Patients
Enrollment of patients • Baseline assessment • Demographic information • Clinical examination • Randomization • Done in 3 unequal blocks of 4, 6 & 8 in a larger block of 18. • Provided with unique ID • NP swab to isolate Spn and Hi.
Study Medicine • Two bottles for each patients • Blue cap – 1st three days • Contained cotrimoxazole • 1st dose given at health care • The cup was marked for the respective patient • to prevent possible mistakes. • White Cap – Last two days • Contained either • contrimoxazole (5 days group) or placebo (3 days group).
Follow up • Follow up on day 3, 5 and 15. • Children were assessed clinically • Compliance to therapy was recorded. • Drug consumption >80% - Medicine was measured • Not missed >1 dose – Marked cells • Outcome recorded • Resolved – on day 3 & 5 • Failed – day 3 & 5 • Relapsed – day 15 • 2nd NP swab was collected on day 15.
Outcome of treatment • Treatment failure on day 3 (any two of the following) • RR is not reduced by 5 • Temp not reduced by 10C • Mother/caregiver mentioned that baby has deteriorated. • Treatment failure on day 5 • RR is fast • Chest in-drawing • Other danger sign(s) • Relapse: Day 15 • Development of pneumonia again by 15 day. • Clinically resolved • RR age specific cut offs • No danger sign
Analysis • Study Population: 2022 under five non severe pneumonia cases were enrolled. • Data were entered in duplicate and verified in EPI Info 6. • Final analysis was done using EPI Info 6 and SPSS 11.0
Number randomized (2022) Day 5 N= 1014 Day 3 N= 1008 Intention to treat analysis Number excluded : -Lost to follow up D5 (LFU) (63) -Protocol violation (PV) (44) Combination LFU and PV (22) Number excluded : -Lost to follow up D5 (LFU) (82) -Protocol violation (PV) (44) -Combination LFU and PV ( 16) Day 3 Followup Number futher analyzed (872) Number futher analyzed (879) Per Protocol analysis Number failed therapy/died 12/0 Number failed therapy/died 18/0 Number improved (854) Number improved (867) Day 5 Followup Number failed therapy/died 64/1 Number failed therapy/died 68/0 Number resolved (790) Number resolved (799) Day 15 Follow-up Number relapsed (55) Number relapsed (62) Number cured (735) Number cured (737)
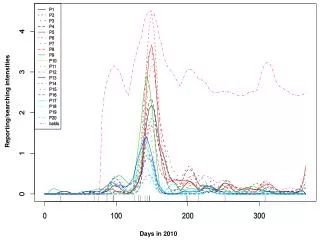
Impact of in vitro resistance on nasal carriage eradication. **100 pairs (persisted) strains were serotyped 85 were found to be identical.
Impact of in vitro resistance on nasal carriage eradication.
Conclusions • Cotrimoxazole therapy for 3 and 5 days are equivalent. • Treatment with cotrimoxazole increases the nonsusceptibility of NP carriage strains. • Impact of treatment on carriage strains is proportionate with the duration of therapy. • As a whole, short course cotrimoxazole is effective in a population with high rate of in vitro non susceptible Spn and Hi with reduced impact on carriage strains.
Impact of treatment on nasal isolates perprotocol cases: S. pneumoniae
Impact of treatment on nasal isolates perprotocol cases: H. influenzae
COTRIMOXAZOLE STUDY GROUP MEMBERS • INDONESIA • Cissy B. K • Dwi Agustian • Chrysanti • Ni Sayu Dewi • Maula Rifada • Anglita • Vidi Permatagalih • Sri Yusnita • BANGLADESH • Samir K. Saha • Nawshad • M. Hanif • M. Ruhulamin • Billal Hossain • Rafeza Khanam • Tanima Sharmin • Maksuda Islam • Abdullah-Al-Mahin • Masoodul Haque • Shams-el Arifeen CONSULTANTS Eric Simoes, MD. Shamim Qazi, WHO