Download
1 / 41
420 likes | 736 Views
Positron Emission Tomography (PET) Jann Mortensen Department of Nuclear Medicine & PET, Rigshospitalet, Copenhagen, Denmark. E-mail: jannmortensen@rh.dk. 8th Annual Congress, Thoracic imaging in lung diseases, April 30th 2005. annihilation photon. g. electron/positron annihilation. b -.

E N D
Positron Emission Tomography (PET) Jann Mortensen Department of Nuclear Medicine & PET, Rigshospitalet, Copenhagen, Denmark E-mail: jannmortensen@rh.dk 8th Annual Congress, Thoracic imaging in lung diseases, April 30th 2005
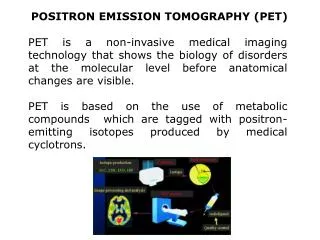
annihilation photon g electron/positron annihilation b- b+ g annihilation photon Decay with positron emission Princip of Positron Emission Tomography Radioactive glucose ligand: 18Fluoro-Deoxy-Glucose 1+ 0.0 (109.77m) EC1, 0+ 0.0 (stable)
Normal cells use glucose GLU GLU GLU-6-phoshate CO2+H20 hexokinase FDG FDG-6- phoshate FDG Glut 1 & 3
(Warburg O. 1930, 129-169) Cancer cells use much glucose * Also high amino acid and nucleic acid use GLU GLU GLU-6-phoshate CO2+H20 FDG FDG-6- phoshate FDG Metabolic trapping Glut 1 & 3
Physiology of FDG tumor uptake FDG signal in tumor is dependent on 1) delivery (blood flow), 2) transport into the cells, and 3) phosporylation FDG tumor uptake ~ number of viable cancer cells
Normal FDG-PET • Visual assessment
Physiologic and patologic FDG metabolism • SUV (standard uptake value) = tumor uptake in relation to mean body uptake • Correlates with degree of malignancy • (Cut-off value > 2.5 SUV ~ malignancy) MIP 3-D projection Colour scale ~SUV
Prognostic information from tumor metabolism PET predicts survival SUV Median survival low uptake < 10 2 yr high uptake > 10 1 yr + large mass >3 cm ½ yr Ahuja et al. Cancer 1998; 83 ; 918-24 In multivariate analysis,the SUV was independently predictive of disease-free and overallsurvival Vansteenkiste J, Fischer BM, Dooms C, Mortensen J. Lancet Oncol 2004; 5: 531–40
Performing a PET study • Patient preparation: > 4 h fast, drink (but no sugar) • Blood sample for glucose (no hyperglycaemia) • 400 MBq 18-F FDG i.v., rest ½-1 h • Scan time: • PET: regional ~ 15-30 min, whole body scan 60 min • PET/CT: regional < 15 min, whole body scan <30 min PET CT
Low dose CT PET Fused PET + CT
CT PET Fused PET + CT Anato-metabolic imaging
Cancer Infection & inflammation Indications: PET in pulmonary disease
Cancer @ Pulmonary nodules Staging (NSCLC) Relaps and re-staging Treatment monitoring SCLC Mesothelioma [Radiation field planning] Indications: PET in pulmonary disease @ PET costs covered by US Medicare
Cancer @ Pulmonary nodules Staging (NSCLC) Relaps and re-staging Treatment monitoring SCLC Mesothelioma [Radiation field planning] Infection & inflammation* Localisation and monitoring of activity: Sarcoidosis AIDS (opportunistic infections and malignancy) Fever of unknown origin Lung abscess Tuberculosis, Actinomycosis, Histoplasmosis, Invasive aspergillosis Vasculitis (Wegener, Takayasu..) Radiation induced inflammation Indications: PET in pulmonary disease @ PET costs covered by US Medicare * = Sem Nucl Med 2002 ;32: 293-321
Main indication: FDG-PET in SPN • Single pulmonary nodule/mass on CT which is borderline for malignancy • cannot be easily biopsied or inconclusive biopsy • Malignant or benign ? • Indication supported by > 16 studies in > 1000 patients with histologic/long-term follow-up • Sensitivity 0.96 • Specificity 0.78 • PPV and NPV >0.90 • Size: 1-4 cm • 1474 nodules (JAMA 2001; 285: 914-24) • Only 8 nodules <1 cm: 3 TP, 2 TN, 3 FN • Diagnostic value in < 1 cm small nodules ? Lancet Oncol 2001;2:659-66
Case 1: 57 y-o-m with COPD 9 mm nodule found on high-resolution CT 18F-FDG PET
Case 1: 57 y-o-m with COPD transaxial coronal saggital Diagnosis and staging (PET suggests T1 N0 M0) attenuation corrected RH - PET / jm (ap)
FDG PET in small nodules (<10 mm) • The interpretation of FDG-PET findings in subcentimetric nodules is at present unsolved. • [Vansteenkiste JF. Lung Cancer 2004; 45: 29-30]. • 4 new studies on > 100 SPN in the litterature • 3 positive and 1 negative about the value of FDG PET • [Lung Cancer 2004; 45:19—27] [Nucl Med Commun 2004; 25: 3-9] • [Am J Respir Crit Care Med. 2005 (in press)][Lancet 2003;362:593-79] Studies in progress on value of PET in low-dose CT screening
FDG PET in large nodules • FDG-PET can discriminate between malignant / benign ≥ 10 mm solid pulmonary nodules ! • FDG-PET has a high negative predictive value, can correctly exclude malignancy in the vast majority of nodules seen in daily practice. • A surgical procedure can be avoided, • A repeat CT after 3-12 months can be used to confirm the absence of growth (ie. benignity). Lancet Oncol 2001; 2: 659-66 Lung Cancer 2004; 45: 29-30.
Main indication : Staging in NSCLC T NM status (in one exam.) • Conventional staging is inaccurate. After presumably radical treatment, 20% develop an early distantrelapse. • [Lancet 1996;347:649–653]. Indication supported by studies in > 1500 patients with histologic/long-term follow-up Lancet Oncol 2001;2:659-66
Impact of PET in lung cancer • PET changes stage in 35% of patients (N=894, 16 studies) • Usually the PET stage is higher than with usual work-up incl. CT • Due to local (N2 eller N3) metastasis or extra-pulmonary metastasis • ie. operation is unnecessary • change in therapy to chemotherapy and / or radiation treatment • Semin Nucl Med 2002, 32:240-71 • PET is cost effective in lung cancer • Both for diagnosis of single pulmonary nodules and for Staging • References: (Gambhir J Clin Oncol 1998; 16: 2113-2125) (Dietlein Eur J Nucl Med 2000; 27: 1441-56) (Gould ARRDCCM 2001) (Plus study)
Randomised study of PET staging • Effect parameter: no. unneccesary thoracotomy´s • 188 ptt. usual work-up +/- PET, 1 yr follow-up • 9 Deutch hospitals (1 dedicated PET center) • PET reduced the no. unneccesary thoracotomy´s: • PET 32 (41%) , + PET 18 ptt (21%) • For each 5 PET scans one unneccesary thoracotomy was avoided • reduced cost per patient with PET: > 1.000 EURO (PLUS study. Lancet 2002; 359: 1388-92)
Prospective study of preoperative staging with PET vs. standard staging (CT, ultrasound, bone scanning) • 102 patients with resectable NSCLC, 6 months follow-up, • histopathological reference. • (N) metastasisSensitivitySpecificity • PET 91 % 86 % • CT 75 % 66 % (M) metastasis: PET identified distant metastases not found by standard methods in 11 of 102 patients: PET identified a different stage in 62 patients: stage was lowered in 20 and raised in 42 Pieterman et al. N Engl J Med 2000;343:254-61
FDG PET for extrathoracic metastasis • 40% with NSCLC have distantmetastases at presentation, most often in the • adrenal glands,bones, liver, or brain [Ann Thorac Surg 1996;62:246–250]. • Adrenal glands: 10% of NSCL have enlarged adrenal glands on CT, 2/3 being benign. • PET has high sensitivity (>92%) and specificity (80%–100%) -> reduces number of unnecessary adrenal biopsies. • Bone: Bone scintigraphy good sensitivity (90%), low specificity (±60%), • PET good sensitivity (90%), but higher specificity (98%)and accuracy (96%). • Liver:US and/or CT remain thestandard imaging techniques for the liver. No good comparisons studies. Additional diagnosticinformation by PET combined with CT, in thedifferentiation of hepatic lesions that are indeterminate onconventional imaging. • Brain:PET low sensitivity (60%) not suited for the detection of brain metastases. The Oncologist 2004; 9 (6): 633-43
FDG PET for extrathoracic metastasis • 40% with NSCLC have distantmetastases at presentation, most often in the • adrenal glands,bones, liver, or brain [Ann Thorac Surg 1996;62:246–250]. • Adrenal glands: 10% of NSCL have enlarged adrenal glands on CT, 2/3 being benign. • PET has high sensitivity (>92%) and specificity (80%–100%) -> reduces number of unnecessary adrenal biopsies. • Bone: Bone scintigraphy good sensitivity (90%), low specificity (±60%), • PET good sensitivity (90%), but higher specificity (98%)and accuracy (96%). • Liver:US and/or CT remain thestandard imaging techniques for the liver. No good comparisons studies. Additional diagnosticinformation by PET combined with CT, in thedifferentiation of hepatic lesions that are indeterminate onconventional imaging. • Brain:PET low sensitivity (60%) not suited for the detection of brain metastases. The Oncologist 2004; 9 (6): 633-43
PET/CT in lung cancer ”PET/CT will improve staging in 20- 40 % of lung cancer patients” Lardinois D et al. N Engl J Med 2003; 348: 2500-7 Cerfolio RJ et al. Ann Thorac Surg 2004; 78: 1017–23 A randomised study in progress in Copenhagen
Value of PET in lung cancer • Sensitivity ~ 96 % (SPN); ~ 73% (N staging) • Specificity ~ 78 % (SPN), ~ 93% (N staging) • Reasons for false negative • Small size (resolution 6 mm, movement) • Well-differentiated tumors: • Adenocarcinoma • Carcinoids (Neuroendocrine tumors) • Broncioalveolar carcinoma (BAC) • Dysregulated diabetes, insufficient fast • Reasons for false positive • Infection / inflammation (Indication per se)
Increased FDG-PET uptake can be seen inbenign pulmonary conditions • Infections • Lung abscess • Tuberculosis (and M avium intracellulare) • Bacterial pneumonia, Actinomycosis, Histoplasmosis, Invasive aspergillosis, aspergilloma, blastomycosis • Inflammatory lesions • Sarcoidosis • Vasculitis: Wegeners granulomatosis, takayasu arteritis, etc • Pneumoconiosis (silicosis, coal workers-, fibrosis) • Rheumatoid arthritis, sclerosing mediastinitis • Amyloidosis, Idiopathic pulmonary fibrosis • Bronciolitis oblitarative organising pneumonia (BOOP),etc • Benign neoplasm (-chondrohamartoma) • Iatrogenic disorders • Radiation induced pneumonitis, biopsy, rib fractures, etc Case stories Sem Nucl Med 2002;32(4):246 & 293-321
Increased FDG-PET uptake can be seen inbenign mediastinal adenopathies(Z) • Granulomatosis and silicosis (Inflammation) • Sarcoidosis • Anthrasilicosis • Infections • Histoplasmosis, • Tuberculosis (and M avium intracellulare) • Actinomycosis, etc. • Benign neoplasm (-thymoma, teratoma, swannoma) • Iatrogenic disorders (Radiation related changes) Case stories (Z) Yet, only a minority with these conditions have a high FDG uptake Sem Nucl Med 2002;32(4): 293-321
FDG PET in active tuberculosis • TB in a 58-year-old man. (A) chest radiograph shows two nodules (b) coronal FDG PET scan shows increased uptake (solid arrow) in the left upper lobe nodules (SUV 4). • Radiology 2000 6:117-21
Sarcoidosis Monitoring: Localisation of activity in- and outside lungs: Before treatment: After inhaled steroid: After prednisolone: • Milman N, Mortensen J, Sloth C. Respiration. 2003;70:408-13.
Newer indications for PET in lung cancer PET predicts survival SUV median survival < 10 2 yr > 10 1 yr + mass >3 cm ½ yr Ahuja et al. Cancer 1998; 83 ; 918-24 • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging and diagnosis of Mesothelioma
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging and diagnosis of Mesothelioma
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging and diagnosis of Mesothelioma • PET/CT guided RT improves radiation dose to the tumor • and metastases and reduces dose to adjacent normal tissue • No studies with patient outcome yet
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging and diagnosis of Mesothelioma
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging and diagnosis of Mesothelioma J Nucl Med. 1999 Aug;40(8):1241-5. Semin Oncol. 2002 Feb;29(1):26-35. • FDG PET for: • Guiding of biopsy • Staging (extrathoracic or contralateral metastasis)
Help from a PET-scan • A positive PET focus indicates malignancy • but needs histological proof (to avoid false positive) • PET or PET/CT guided biopsy possible • A negative PET focus indicates benignancy • A solitary pulmonary nodule is either benign or very slowly growing cancer (no or CT control 6-12 months for growth) • Staging, no metastasis found, refer to operation.
Conclusion • Single Pulmonary Nodules • Differentiate between benign/malignant indeterminate SPN • if biopsy is difficult / nondiagnostic • confirm benignity with CT follow-up • the uptake predicts prognosis (high metabolism -> bad prognosis) • StagingRegional (N) and distant (M) metastases: • Addition of PET improves conventional staging (CT+US+ bone scintigraphy) • PET changes stage and treatment in ~35 % of patients • Detects unexpected distant metastases in ~14 % • Exclusion of malignancy in ~5 % (can be operated) • Usually a higher stage is found • Avoids unneccesary thoracotomy (in 10-20 %) • Mediastinoscopy can be avoided if PET + CT are normal (in non-central tumors) • Other indications: • Restaging and treatment monitoring, radiation field planning, SCLC, Mesothelioma • Localisation & monitoring of infections & inflammatory disorders