Download
1 / 20
220 likes | 579 Views
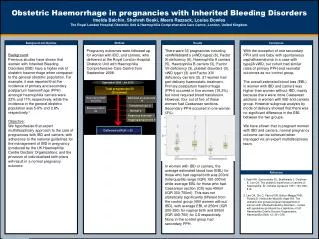
Severe Obstetric Haemorrhage. Max Brinsmead PhD FRANZCOG March 2010. Introduction. The average gravida carries 1 - 1.5 l of “extra blood” in pregnancy as prophylaxis against PPH but… PPH is a major cause of obstetric death especially in 3rd world countries

E N D
Severe Obstetric Haemorrhage Max Brinsmead PhD FRANZCOG March 2010
Introduction • The average gravida carries 1 - 1.5 l of “extra blood” in pregnancy as prophylaxis against PPH but… • PPH is a major cause of obstetric death especially in 3rd world countries • 10 - 15% of women lose >600 ml of blood at delivery and… • For 1 - 2% the blood loss can be life threatening • Another 0.5 - 1% have severe antepartum haemorrhage from abruption or placenta previa
This presentation will address… Emergency (First aid) and Diagnosis and management of severe APH Advanced Measures for the management of excessive blood loss in the first 24 hours after birth
Risk factors for Primary PPH • Prolonged labour • APH • Pre eclampsia • Maternal obesity • Multiple pregnancy • Birth weight >4000g • Advanced maternal age • Previous PPH • Assisted delivery • Low lying placenta • But >50% occur in women without identified risk factors and… • 90% are associated with uterine atony • And all studies of massive PPH fail to identify consistent risk factors
Patient Assessment • Objective measure of blood loss is desirable • Postural hypotension the earliest sign • Tachycardia is usual • Air hunger and loss of consciousness is serious • Urine output a good measure of treatment • CVP sometimes • A bedside test of blood clotting desirable
Emergency Measures for PPH • Rub up a contraction • Deliver the placenta • If you can • Gain IV access (large bore cannula) • Additional oxytocic • IV Ergometrine 0.25 mg • Syntocinon infusion • Rectal Cervagem or Misoprostol • (Empty the bladder) • Bimanual uterine compression • Aortic compression
Advanced Measures 1 • Get help • Check coagulation - use cryoprecipitate etc. • EUA is mandatory • Myometrial PG F2 alpha • Uterine Packing • Intrauterine balloon catheter • Consider activated Factor VII
Blood replacement products: • Whole blood All components (after 48hrs factors low) • Packed Red cells Red cells only • Frozen plasma All clotting factors except for platelets Store up to 1 year at -20 to -30 C • Cryoprecipitate Fibrinogen, factors VIII, XIII, VWF lacks antithromin III • Platelets Only last 5 days
The Coagulation Mechanism • Mechanical • Contraction • Surgical • Coagulation Cascade • Platelet plug • Clotting cascade • Thrombin > Fibrinogen to Fibrin • Termination • Removal
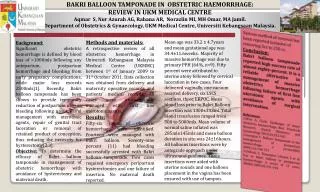
Intrauterine Balloon Tamponade BJOG Review May 2009 Was effective in 91.5% of cases Combined retrospective and prospective studies But only a total of 106 patients Types of balloons Sengstaken Blakemore (GI use) Rusch (Urological) Foley (often multiple) Bakri (Specifically designed for obstetrics) Condom (+/- Foley) But there remain many unanswered questions
Questions concerning intrauterine balloon tamponade BJOG Review May 2009 Is it effective There are no RCTs Risks and contraindications Which balloon to use, how to insert it and what volume to inflate it Is a vaginal pack required Is an oxytocin infusion required Antibioitics and analgesia When to deflate and or remove it
Advanced Measures 2 • Get more help • Medical – haematologist • Surgical colleague • Radiologist for… • Uterine artery embolisation • Laparotomy and… • B-Lynch suture • Internal iliac artery ligation • Aortic clamping • Hysterectomy
When confronted with a pregnant patient who is bleeding after 20w • There are five questions that need urgent answers… • How much blood has been lost • What is the maternal condition • What is the fetal condition • Is the patient in labour • What is the cause of the bleeding
THINK in terms of aetiology... • Bleeding from a normally situated placenta = Abruption • Bleeding from a low placenta = Placenta previa • Cervical bleeding: • “Show” • Ectropion or Cancer
ACT in terms of priority... • Assess maternal wellbeing • Resuscitate if required • Anticipate further problems • Assess fetal wellbeing • Is the fetus compromised • Is the fetus salvageable • Then attempt diagnosis
Essential observations • Maternal vital signs • General appearance • Pulse and BP • Uterus • Size • Tone and tenderness • Contractions • You can’t do this with CTG belts in place • Nature and amount of PV loss • Just blood or blood and liquor • Fetus • Fetal heart present or absent
Essential Investigations • HB, Blood group and save or Xmatch • Depends on the amount of blood lost • And the suspected diagnosis • Remember that abruption is often associated with a large concealed loss • Ultrasound • Best done “on the ward” if bleeding is substantial • Requires skill in distinguishing blood clot from placenta • Vaginal scan the best way of evaluating degrees of placenta previa • Urinalysis for proteinuria • May require bladder catheterisation • Abruption may be associated with “acute” pre eclampsia • And the blood pressure may not be raised
Immediate management • Large bore IV line • If estimated loss is >250 ml • Or if abruption or placenta previa is diagnosed • Resuscitate with IV Fluids • Commence with saline • Colloids if shocked • Blood if estimated loss >2 L • Analgesia • Corticosteroids for gestation <37wks
Monitoring response • Maternal PR and BP • Watch for pre eclampsia • Indwelling catheter • Hourly urine output • Only a few require CVP • Watch for coagulopathy • A bedside test of clotting • Prothrombin time (aPTT) and platelets • HB takes a while to adjust • CTG and umbilical Dopplers for the fetus
Definitive management • Conservative for placenta previa • Most will settle • Deliver when paediatric resources permit • But must proceed to CS at any gestation if the blood loss is life threatening for the mother • Aggressive management for abruption • CS sooner rather than later for fetal reasons • But vaginal delivery is usually possible with IUFD • Give more blood than you see • Watch for coagulopathy