Download
1 / 17
200 likes | 574 Views
Major Obstetric haemorrhage. Miss Melanie Tipples. Objectives. Understand the definition and causes of major haemorrhage Recognise and manage a collapse from haemorrhage Understand the surgical and pharmacological options for management of haemorrhage. Haemorrhage.

E N D
Major Obstetric haemorrhage Miss Melanie Tipples
Objectives Understand the definition and causes of major haemorrhage Recognise and manage a collapse from haemorrhage Understand the surgical and pharmacological options for management of haemorrhage
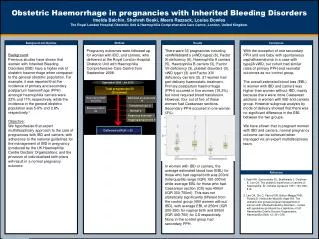
Haemorrhage Major cause of morbidity and mortality for all pregnant women through pregnancy and in post partum period Reduction in deaths in last triennial report but still major cause of death Substandard care found in 3 out of five cases (no obs, concealed bleeding not considered) MEOWS charts for 24 hours post section and need for action where abnormalites found
Definition Major Obstetric Haemorrhage is defined as the loss of more than 1000mls of blood either antepartum or post partum
Causes T – Tone (multiple causes both fetal and maternal) T – Tissue Retained tissue (placenta or products) T - Trauma Genital tract injury, broad ligament haematoma, uterine rupture T- Thrombin ie coagulopathy secondary to haemorrhage, abruption, sepsis, eclampsia or dead fetus, amniotic fluid embolus It can be caused by one or more of the above
Management Identifying you have a problem – look for signs of shock (concealed or revealed) Pulse, respiratory rate, peripheral perfusion, urine output Remember blood pressure drops late Acidosis and confusion/drowsy
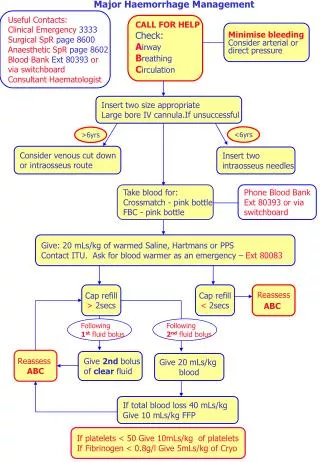
Management Communication and documentation Call for help Resuscitation (ABC) Fluid replacement Arresting the bleeding and obstetric intervention Monitoring and investigation Anaestheticinpurt
TEAM APPROACH MAJOR OBSTETRIC HAEMORRHAGE CALL Make sure you know what that means in your hospital Allocate a team leader
Rescucitation A – Oxygen B – Assess C – two large bore cannulas (grey) and take bloods for FBC, u&es, coag, and cross match. Commence ward colloid infusion Place on oximeter, BP cuff, Insert catheter
Management -Tone Bimanual compression of uterus Empty bladder
Tone - pharmocology Syntocinon 5 units Ergometrine 0,5mg iv/im Sytocinon 40 in 500mls n/saline Carboprost 0.25mg im every 15 minutes to a max of 8 injections Misoprostol 600 microgrammes oral or pr (asthma or home deliveries)
Tone – surgical tecniques Tamponade balloon Haemostatic brace lynch suture Selective arterial embolization
Management - Tissue Failure to respond to pharmolocogical techniques, intermittent relaxation or suspicion that the placenta is incomplete should prompt examination of the uterine cavity under anaesthetic
Management - Trauma Surgical exploration and repair If repair not possible Hysterectomy may be indicated Timely definitive surgery has been shown to be associated with best outcome
Management - Thrombin Involve Haematologist and MLSO early Update them regularly Remember to stand them down
Post Haemorrhage Documentation Datix Debrief Follow up patient and arrange support
Summary Systematic approach and team working has been shown to improve outcome in the most recent CMACE report