Download
1 / 1
10 likes | 121 Views
Language Access Survey. Angela Tobin 1 , Suzanne Bronheim 2 , and Wendy Jones 3. 1 American Academy of Pediatrics, National Center for Medical Home Implementation , 2 & 3 National Center for Cultural Competence, Georgetown University Center for Child & Human Development.

E N D
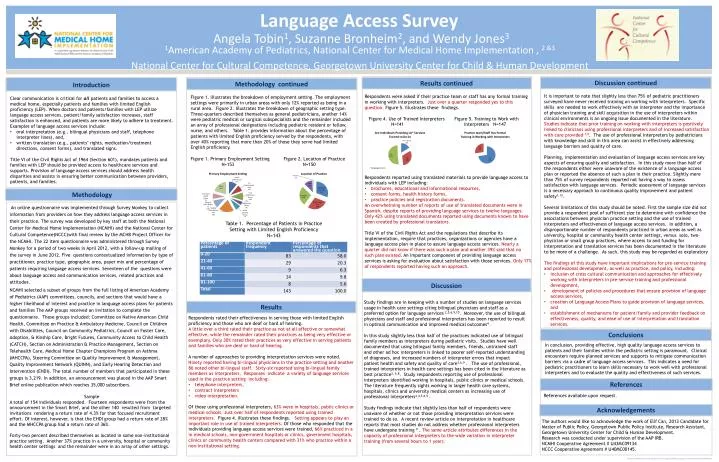
Language Access Survey Angela Tobin1, Suzanne Bronheim2, and Wendy Jones3 1American Academy of Pediatrics, National Center for Medical Home Implementation , 2 &3 National Center for Cultural Competence, Georgetown University Center for Child & Human Development Discussion continued Results continued Introduction Methodology continued Figure 1. illustrates the breakdown of employment setting. The employment settings were primarily in urban areas with only 12% reported as being in a rural area. Figure 2. Illustrates the breakdown of geographic setting type. Three-quarters described themselves as general pediatricians, another 14% were pediatric medical or surgical subspecialists and the remainder included an array of professional designations including pediatric resident or fellow, nurse, and others. Table 1. provides information about the percentage of patients with limited English proficiency served by the respondents, with over 40% reporting that more than 20% of those they serve had limited English proficiency. Figure 1. Primary Employment Setting Figure 2. Location of Practice N=153 N=150 Clear communication is critical for allpatients and families to access a medical home, especially patients and families with limited English proficiency (LEP). When doctors and patients/families with LEP utilize language access services, patient/family satisfaction increases, staff satisfaction is enhanced, and patients are more likely to adhere to treatment. Examples of language access services include: oral interpretation (e.g., bilingual physicians and staff, telephone interpreter lines), and, written translation (e.g., patients’ rights, medication/treatment directions, consent forms), and translated signs. Title VI of the Civil Rights Act of 1964 (Section 601), mandates patients and families with LEP should be provided access to healthcare services and supports. Provision of language access services should address health disparities and assists in ensuring better communication between providers, patients, and families. • It is important to note that slightly less than 75% of pediatric practitioners surveyed have never received training on working with interpreters. Specific skills are needed to work effectively with an interpreter and the importance of physician training and skill acquisition in the use of interpreters within clinical environments is an ongoing issue documented in the literature. Studies indicate that prior training on working with interpreters is positively linked to clinicians using professional interpreters and of increased satisfaction with care provided 7,8. The use of professional interpreters by pediatricians with knowledge and skill in this area can assist in effectively addressing language barriers and quality of care. • Planning, implementation and evaluation of language access services are key aspects of ensuring quality and satisfaction. In this study more than half of the respondents either were unaware of the existence of a language access plan or reported the absence of such a plan in their practice. Slightly more than 75% of survey respondents reported not having a way to assess satisfaction with language services. Periodic assessment of language services is a necessary approach to continuous quality improvement and patient safety1,12. • Several limitations of this study should be noted. First the sample size did not provide a respondent pool of sufficient size to determine with confidence the associations between physician practice setting and the use of trained interpreters and effectiveness of language access services. In addition, a disproportionate number of respondents practiced in urban areas as well as university, hospital or community health center settings, versus solo, two-physician or small group practices, where access to and funding for interpretation and translation services has been documented in the literature to be more of a challenge. As such, this study may be regarded as exploratory • The findings of this study have important implications for pre-service training and professional development, as well as practice, and policy, including: • inclusion of cross cultural communication and approaches for effectively working with interpreters in pre-service training and professional development, • development of policies and procedures that ensure provision of language access services, • creation of Language Access Plans to guide provision of language services, and • establishment of mechanisms for patient/family and provider feedback on effectiveness, quality, and ease of use of interpretation and translation services. • Respondents were asked if their practice team or staff has any formal training in working with interpreters. Just over a quarter responded yes to this question. Figure 5. Illustrates these findings. • Figure 4. Use of Trained Interpreters Figure 5. Training to Work with • N=141 Interpreters N=147 • Respondents reported using translated materials to provide language access to individuals with LEP including: • brochures, educational and informational resources, • consent forms, health history forms, • practice policies and registration documents. • An overwhelming number of reports of use of translated documents were in Spanish, despite reports of providing language services to twelve languages. Only 42% using translated documents reported using documents known to have been created by professional translators. • Title VI of the Civil Rights Act and the regulations that describe its implementation, require that practices, organizations or agencies have a language access plan in place to assure language access services. Nearly a quarter did not know if there was such a plan and another 39% said that no such plan existed. An important component of providing language access services is asking for evaluation about satisfaction with those services. Only 17% of respondents reported having such an approach. Study findings are in keeping with a number of studies on language services usage in health care settings citing bilingual physicians and staff as a preferred option for language services 2,5,6,9,10. Moreover, the use of bilingual physiciansand staff and professional interpreters has been reported to result in optimal communication and improved medical outcomes4 . In this study slightly less than half of the practices indicated use of bilingual family members as interpreters during pediatric visits. Studies have well documented that using bilingual family members, friends, untrained staff and other ad hoc interpreters is linked to poorer self-reported understanding of diagnoses, and increased numbers of interpreter errors that impact patient health and safety and quality of care3,6,9 . The use of professional, trained interpreters in health care settings has been cited in the literature as best practice3, 6,8. Study respondents reporting use of professional interpreters identified working in hospitals, public clinics or medical schools. The literature frequently sights working in larger health care systems, hospitals, clinics and university medical centers as increasing use of professional interpreters2,4,5,6,9 . Study findings indicate that slightly less than half of respondents were unaware of whether or not those providing interpretation services were trained to do so. A recent review article on interpretation in healthcare reports that most studies do not address whether professional interpreters have undergone training 9 . The same article attributes differences in the capacity of professional interpreters to the wide variation in interpreter training (from several hours to 1 year). Methodology An online questionnaire was implemented through Survey Monkey to collect information from providers on how they address language access services in their practice. The survey was developed by key staff at both the National Center for Medical Home Implementation (NCMHI) and the National Center for Cultural Competence(NCCC)with final review by the MCHB Project Officer for the NCMHI. The 22 item questionnaire was administered through Survey Monkey for a period of two weeks in April 2012, with a follow-up mailing of the survey in June 2012. Five questions contextualized information by type of practitioner, practice type, geographic area, payer mix and percentage of patients requiring language access services. Seventeen of the questions were about language access and communication services, related practices and attitudes. NCMHI selected a subset of groups from the full listing of American Academy of Pediatrics (AAP) committees, councils, and sections that would have a higher likelihood of interest and practice in language access plans for patients and families The AAP groups received an invitation to complete the questionnaire. These groups included: Committee on Native American Child Health, Committee on Practice & Ambulatory Medicine, Council on Children with Disabilities, Council on Community Pediatrics, Council on Foster Care, Adoption, & Kinship Care, Bright Futures, Community Access to Child Health (CATCH), Section on Administration & Practice Management, Section on Telehealth Care, Medical Home Chapter Champions Program on Asthma (MHCCPA), Steering Committee on Quality Improvement & Management, Quality Improvement Network (QUINN), and Early Hearing Detection and Intervention (EHDI). The total number of members that participated in these groups is 3,219. In addition, an announcement was placed in the AAP Smart Brief online publication which reaches 35,000 subscribers. Sample A total of 154 individuals responded. Fourteen respondents were from the announcement in the Smart Brief, and the other 140 resulted from targeted invitations rendering a return rate of 4.3% for that focused recruitment effort. Of interest, however, is that the EHDI group had a return rate of 28% and the MHCCPA group had a return rate of 36%. Forty-two percent described themselves as located in some non-institutional practice setting. Another 37% practice in a university, hospital or community health center settings and the remainder were in an array of other settings. Table 1. Percentage of Patients in Practice Setting with Limited English Proficiency N=143 Discussion Results • Respondents rated their effectiveness in serving those with limited English proficiency and those who are deaf or hard of hearing. • A little over a third rated their practice as not at all effective or somewhat effective, while the remainder rated their practices as being very effective or exemplary. Only 30% rated their practices as very effective in serving patients and families who are deaf or hard of hearing. • A number of approaches to providing interpretation services were noted. Ninety reported having bi-lingual physicians in the practice setting and another 86 noted other bi-lingual staff. Sixty-six reported using bi-lingual family members as interpreters. Responses indicate a variety of language services used in the practice setting including: • telephone interpreters, • contract interpreters • video interpretation. • Of those using professional interpreters, 63% were in hospitals, public clinics or medical schools.Just over half of respondents reported using trained interpreters. Figure 4. illustrates these findings. Setting appears to play an important role in use of trained interpreters. Of those who responded that the individuals providing language access services were trained, 66% practiced in a in medical schools, non-government hospitals or clinics, government hospitals, clinics or community health centers compared with 31% who practice within a non-institutional setting. Conclusions In conclusion, providing effective, high quality language access services to patients and their families within the pediatric setting is paramount. Clinical encounters require planned services and supports to mitigate communication barriers via a cadre of language access services. This indicates a need for pediatric practitioners to learn skills necessary to work well with professional interpreters and to evaluate the quality and effectiveness of such services. References References available upon request. Acknowledgements The authors would like to acknowledge the work of Elif Can, 2013 Candidate for Master of Public Policy, Georgetown Public Policy Institute, Research Assistant, Georgetown University Center for Child & Human Development. Research was conducted under supervision of the AAP IRB. NCMHI Cooperative Agreement # U43MC09134 NCCC Cooperative Agreement # U40MC00145.