Download
1 / 13
130 likes | 138 Views
Learn about diagnosis and management strategies for diabetic eye diseases including cranial neuropathy, glaucoma, retinal vascular occlusions, and related macrovasculopathy. Understand the impact of diabetes on eye health and preventive measures. Stay informed for better eye care.

E N D
Diagnosis & Management of Diabetic Eye Disease Part 4 A. Paul Chous, M.A., O.D., F.A.A.O. Tacoma, WA Specializing in Diabetes Eye Care & Education
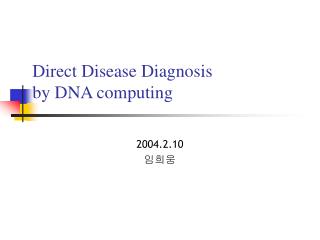
Efferent Cranial Neuropathy • Microvascular infarct commonly leads to short-lived IIIrd, IVth, VIth and VIIth CN palsies • 2-6 month duration • Isolated CN palsy as a rule • Autonomic neuropathy leads to diminished pupillary reflexes and accommodative response
30 minutes Later
Cranial Neuropathy- Management • Improve blood glucose control • Patch/use prism as necessary • Consider earlier use of bifocal correction
Glaucoma • Controversy regarding DM as a risk factor for POAG; undisputed risk for NVG • The Nurses Health Study (n = 76,3180) and meta-analysis of 12 studies (1987-2001) reveal a 50-80% increased risk of POAG in DM Ophthalmology 2006 Jul;113(7): 1081-6 Diabet Med 2004 Jun;21(6): 609-14 • Basic science has shown that AGEs ‘harden’ laminar collagen leading to shear stress • There may be a strong detection bias
Glaucoma - Management • Avoid unnecessarily treating OHTN in patients with diabetes • Increased risk of sight-threatening retinopathy with lower IOP and increased blood flow • Avoid beta blockers in pts on insulin • Increase blood glucose and may cause ‘hypoglycemia unawareness’ • Refer NVI for immediate PRP • Anti-VEGF agents successfully used in 2 cases
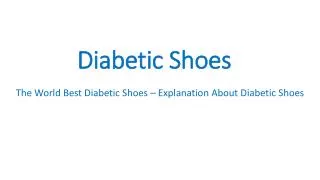
AION • Two-thirds of patients with non-arteritic AION have DM, HTN, or both • Younger patients with T1DM often have good recovery of vision (‘diabetic papillopathy’) – not always the case • PREVENTION: strongly consider ASA therapy for patients with DM and small cups & hyperemic discs (‘disc at-risk’) • Aggresively treat HTN & dyslipidemia Optic disc on Fluorescein Angiography
Retinal Vascular Occlusion • Retinal venous and arterial occlusions are more common in diabetes (especially BRVO) • Increased probability of predisposing factors: • Hypertension • Dyslipidemia • Hypercoagulability Especially in Type 2 Diabetes
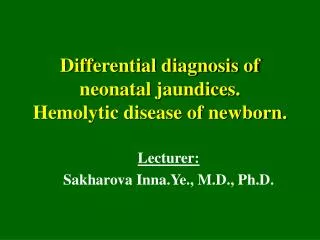
BRVO Sticky Platelets + HTN = Venous Occlusion
Major risk factors for RAOs are hypertension, atherosclerosis & cardiac valve disease – Two of which are more common in diabetes CRAO
Retinal Vascular Occlusion – Prevention & Management • Improve & stabilize blood glucose • Aggressively treat HTN and dyslipidemia • Monitor closely for neovascularization in all venous occlusions associated with diabetes • ‘Double Whammy’ of ischemia from hyperglycemic capillary closure and venous stasis
Macrovasculopathy & Diabetic Eye Disease • DRT, Retinal Vascular Occlusion and AION strongly correlated with systemic CV disease • -Sticky Platelets from hPAI-1 • -Reactive Oxygen Species injure • blood vessel wall • -Embolic Events from rupture of vulnerable plaque due to hCRP