Download

1 / 43
430 likes | 566 Views
STI surveillance Belgium Results and recommandations. Ruth Verbrugge WIV-ISP 10-12-2013 9 th STI-HIV seminar. What ?. Monitoring trends and estimating incidence

E N D
STI surveillance Belgium Results and recommandations Ruth Verbrugge WIV-ISP 10-12-2013 9th STI-HIV seminar
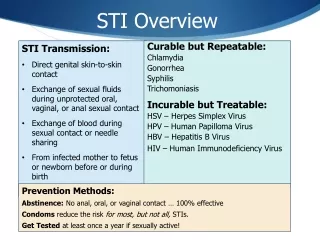
What ? • Monitoring trends and estimating incidence = > sentinel network of laboratories for microbiology • Identifying population groups athigherrisk for specificSTI’s => sentinel network of clinicians
Why ? • Providing essential information for prevention & control • Authorities (Regional, National, Europe, WHO) • Local non-profit organisations • Development, adaptation, finetuning of guidelines • Organisation of orientedfieldactivities
Outline 1. Trends and incidence 2. Population at risk3. What to do?
Chlamydia • Chlamydia is the most frequent reported STI. • The increasing trend continues in 2012. • The increase in Flanders : probablyduetosensibilisationcampaign on testing • The increase in Wallonia : probablydueto attention in newspapersand+ 1university laboratory
Chlamydia • Most affected : women; 15 to 29 yearsold • Man / Women : 1/1,83 • Highestincidence : Brussels andAntwerp, resp.194 and148 cases/100 000 inhab.
Trend in agedistributionfor Chlamydia by gender, Belgium, 2002-2012 WOMENMEN
Trend in agedistributionfor Chlamydia by gender, Belgium, 2002-2012 WOMENMEN
Gonorrhoae • Increasing trend • Most affected : men;15 tot 34 yearsold • Men/women : 3,2/1 • Highestincidence : Brussels andAntwerp, • resp. 39 and 35 cases/100 000 inhabitants • Treatment : first signs of resistencyagainstcefixime(notused in Belgium) andceftriaxone(in othercountriesthan Belgium)
Resistency?What is the best treatment for gonorrhoe? • next speakers
Syphilis • Slower increase since 2009, stabilising in Flanders and Wallonia, further increasing in Brussels • Most affected: men; 25 up to 59 years old • Men/women : 4,8/1 • Highest incidence : Brussels, Arlon and Antwerp, resp. 47, 45 en 33 cases/100 000 inhabitants • Syphilisreinfection(in male) : 26%
Syphilis reinfection Wallonia Belgium Flanders Brussels
What attracks out attention? • Chlamydia => Age • Gonorrhoea => AB- Resistance • Syphilis = > Reinfection
THANKS to the Medical doctors who fill out voluntary the questionnaire for each STI patient
Distribution of registered STI by specialisation of medical centre Mean number of STI registrations by specialisation
Percentage of STI cases diagnosed without STI complaint • Highest% of STI cases diagnosed without STI complaint: • Centresfor FP (80%) • STI clinics (60%) • Gynaecologists (57%) • Lowest% of STI cases diagnosed without STI complaint: • generalists (15%) There are no official screening guidelines. Doctors ask for it, something to hold on and to be aligned.
Observation • 2 gynaecologists: • 57% (48/84) and 55% (27/49) of STI patients found thanks to screening • and 50% of those STI patients were pregnant • 0,6% perinatal Chlamydia-infections ↔ Antenatal screening recommendations for Chlamydia
It is worthwhile to have Chlamydia prevalence trial within the 15-34 year old age group and a revision of antenatal screening recommendations
Partner notification • 44% : YES • 13% : NOT • 6% of STI cases found thanksto partner notification Encourage partner notification => A key factor in prevention
Risk behaviourNumber of sex partners < 6 m prior to the STI diagnosis
Risk behaviourCondom use among registered STI patients 62% never uses a condom 80% did not use a condom during last sexual intercourse
Other risk groups • Commercial sex workers • PWID • Travelling : 5 % of Belgian STI-patients
Overview BEHAVIOUR No condomuse ≥2 sex partners Group sex Oralsex Notnotifyingsex partner Havingsexualcontactsabroad GROUPS Young people Young adults MSM Swingers CommSexworkers PWID
3% of STI patients discovered their HIV+ status together with STI diagnosis • Patients diagnosed with a STI need to be screened for HIV • Patients who ask a HIV test need to be screened for STI
Legitimaterequestfrom the medicalcorps forofficial screening guidelines With a special attention to Chlamydia and gonorroe, because of the asymptomatic course and the fertilityconsequences Heterosexual men andwomen (with or without complaint), worriedafter a sexual contact People who start a new partnership with a new partner With a special attention towards • Adolescentsandyoungadults • Men andwomenwith multiple partners • Men andwomenpracticinggroupsex, inclswingers • MSM with multiple partners, partner exchange, practicinggroupsex • SAM (HIV risk group) • Commercial sexworkers • PWID • Travellerswho had sexual contact abroad, otherthantheir fix partner • Partners of a STI Patient • Pregnant women
With attention to young people IntegrateChlamydia andgonorrhoe screening foryoung men andwomenwithin the current HPV screening recommendationforwomen Extendreimbursment * for Chlamydia screening (NAAT) at leastup to 30 yearsold Extendthe currentprenatalsyphilisandHIV screening recommendation ** withChlamydia andgonorrhoe *Diagnosis role NAAT PCR for Chlamydia: max. twice a yearifpatient is younger or equalto 20 yearsold; or withpresence of specific STI symptoms **Ref KCE report 6A, 2004
THANKS FOR YOUR ATTENTION QUESTIONS?