Download
1 / 13
130 likes | 332 Views
Clinical Case 2. Andrew J Coats Norwich Research Park, Norwich, UK. Relevant disclosure of interest: Consultant to Daiichi Sankyo and the Menarini group. Presentation. Patient requested a specialist consultation

E N D
Clinical Case 2 Andrew J Coats Norwich Research Park, Norwich, UK Relevant disclosure of interest: Consultant to Daiichi Sankyo and the Menarini group
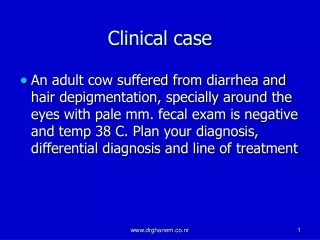
Presentation • Patient requested a specialist consultation • her own self-monitored systolic BP has been consistently above 160 mmHg (which she had read was too high) • she had noticed increasing shortness of breath and early morning wheeze and coughing • GP reassured patient that her BP was adequately controlled because her diastolic BP had mostly been below 80 mmHg
History Taking • Mrs HK is a 74 year old Finnish diplomat’s wife who has lived in London for the last 4 years • She is active • An ex-smoker • Known and treated hypercholesterolaemia • Elevated fasting glucose levels noted recently • Family history: • premature ischaemic heart disease (father and two brothers) • stroke (mother)
History Taking - 2 • 5 years previously she had two TIAs and one more prolonged ischemic episode that left her with a minor expressive dysphasia • She denied recent neurological symptoms • Treatment: • simvastatin 20 mg per day • bendrofluazide 5 mg per day • carvedilol 25 mg bd • enteric coated aspirin 80 mg per day
Question 1 • What diagnoses do you think are likely?
Question 2 • What investigations would you like to see?
Results - 1 • We arranged: • 24 hour BP monitoring • a full metabolic blood profile • echocardiogram • ABPM – BP monitoring showed a substantial white coat alerting response: • clinic BP average = 176/72 mmHg • day time average = BP 154/72 mmHg • sleep average = 130/62 mmHg
Results - 2 • Sodium 144 (136–145) mmol/L • Potassium 3.6 (3.5–5.1) mmol/L • Urea 7.9 (1.7–8.3) mmol/L • Creatinine 95 (44–80) mmol/L • eGFR 75 mL/min/1.73 m2 • Glucose (Fasting) 6.5 mmol/L • HaemoglobinA1c 8.71 (5.5–7.0 %) • Gamma GT 55 (5–36 IU/L) • Cholesterol 5.5 mmol/L • Triglycerides 0.71 mmol/L • HDL Cholesterol 1.77 mmol/L • LDL (Calculation) 3.43 mmol/L • HDL/Cholesterol ratio 0.32 • Cholesterol/HDL ratio 3.11
Treatment • Patient seen in clinic and commenced on ramipril 5 mg bd, which she did not like, as she said it made her feel lethargic, and she complained her cough was a lot worse after the first two days of treatment • Her doctor reassured her these were unlikely to be due to ramipril as the reaction was too quick, but repeat blood tests showed: • Sodium 140 (136–145) mmol/L • Potassium 4.9 (3.5–5.1) mmol/L • Urea 8.9 (1.7–8.3) mmol/L • Creatinine 123 (44–80) mmol/L • eGFR 57 mL/min/1.73 m2
Question 3 • What do you think is happening?
Progress (3 months later) • The patient had stopped the ramiprilherself • Renal ultrasound was requested and showed bilaterally small kidneys but no suggestion of renal artery stenosis • Her bendrofluazide was stopped and ramiprilrechallenged, this time with no significant increase in creatinine • However the patient maintained that the cough worsened again and refused to continue ramipril
Progress (continued) • She was then commenced on olmesartan/HCTZ combination at doses of 40 mg/12.5 mg • Carvedilolwas replaced with nebivolol 5 mg per day • Her breathing improved and the cough disappeared • On direct questioning she admitted she had not taken her medication regularly as she found the evening dose hard to remember and often omitted it • She took her medication regularly only for the few days before each visit to her doctor
Outcome • Her repeat blood tests after 6 months were better: • Urea 8.2 (1.7–8.3) mmol/L • Creatinine 99 (44–80) mmol/L • eGFR 72 mL/min/1.73 m2 • Glucose (Fasting) 5.5 mmol/L • HaemoglobinA1c 7.1 (5.5–7.0 %) • Repeat ABPM showed: • Day time average BP = 146/74 mmHg, Sleep average = 134/72 mmHg • Her breathing had improved and she had recommenced her regular Pilates classes