Download
1 / 36
360 likes | 492 Views
Treatment Issues with Asian-Americans. Daryl Fujii Ph.D., Honolulu Paul Lephuoc, Houston (Intern) and the Multicultural/Diversity Committee (2010-2011) VA Psychology Training Council Contact persons: Daryl Fujii Ph.D., Honolulu (Daryl.Fujii@va.gov)

E N D
Treatment Issues with Asian-Americans Daryl Fujii Ph.D., Honolulu Paul Lephuoc, Houston (Intern) and the Multicultural/Diversity Committee (2010-2011) VA Psychology Training Council Contact persons: Daryl Fujii Ph.D., Honolulu (Daryl.Fujii@va.gov) Rachael Guerra Ph.D., Palo Alto (Rachael.Guerra@va.gov)
Multicultural/DiversityCommittee Committee 2010-2011 Loretta E. Braxton Ph.D., Durham (Co-Chair) Linda R. Mona Ph.D., Long Beach (Co-Chair) Angelic Chaison Ph.D., Houston Daryl Fujii Ph.D., Honolulu Rachael Guerra Ph.D., Palo Alto Jamylah Jackson Ph.D., North Texas Monica Roy Ph.D., Boston Christina Watlington Ph.D., Perry Point Miguel Ybarra Ph.D., San Antonio Susana Blanco Ph.D., Bedford (Postdoc) Nancy Cha, Honolulu (Intern) Paul Lephuoc, Houston (Intern) Katherine Hoerster Ph.D., Long Beach (Postdoc)
Overview • Heterogeneity in Asian-Americans • Asian Ethnic Identity Model (Kim) • Shared values, beliefs, behaviors • Clinical implications • Cultural adaptations for treatment • PMAF model (Hwang) • Addressing shame • Case example • Resources • References
Ethnicity in Veteran Population • In 2009, there were 21.9 million veterans in the United States (Infoplease, retrieved 2011) • African Americans 2.3 million • Hispanic 1.1 million • Asian-Americans 258,000 • American Indian or Alaskan Native 153,000 • Native Hawaii or Other Pacific Islander 30,000 • Non-Hispanic White 17.7 million • Female Veterans 1.5 million • (The numbers for blacks, Asians, American Indians and Alaska Natives, Native Hawaiians and Other Pacific Islanders, and non-Hispanic whites cover only those reporting a single race.)
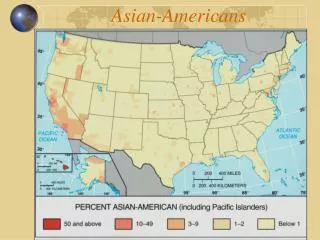
Heterogeneity within Asian-Americans • According to a recent U.S. Census estimates there are about 14.7 million Asian-Americans living in the United States which makes up approximately 4.8% of the population. • 15.3% of Asian-Americans report more than one race (Humes et al., 2011) • 2000 census lists 24 single ethnicities (Reeves & Bennett, 2004): • 1. Chinese (2,422,970 23.8%) -- 7. Cambodian (178,043, 1.8%) • 2. Filipinos (1,864,120 18.3%) -- 8. Hmong (170,049, 1.7%) • 3. Asian Indians (1,645,510 16.2%) -- 9. Laotian (167,792, 1.6%) • 4. Vietnamese (1,110,201 10.9%) -- 10. Pakistani (155,909, 1.5%) • 5. Korean (1,072,682 10.5%) -- 11. Thai (110,851, 1.1%) • 6. Japanese (795,051 7.8%) -- 12. Other (478,363, 4.7%)
Heterogeneity within Asian-Americans • 69% of Asian-Americans are foreign born • Japanese 39% (low) Thais 78% (high) • Decade of highest immigration • Before 1980 (Thai 38%) 1980-1990 (Cambodian 74%) • 1990+ (Pakistanis 59%) • 79% speak a language than English spoken at home • Japanese 47% (low) Hmong 96% (high) • 44% have a Bachelor’s degree or higher • Hmong 7.5% (low) Asian Indians 63.9% (high) • Median family income for all Asians is $59,300 • Hmong $32,384 (low) Japanese $70,849 (high) • (Reeves & Bennett, 2004)
Heterogeneity: Religious Breakdown of Asian-Americans • American Religious Identification Survey 2001, C.N. Le, estimates the religious breakdown among Asian-Americans • 21.1 percent Catholic • 20.2 percent none/agnostic • 9.6 percent Protestant • 9.1 percent Buddhist • 5.8 percent Christian • 5.2 percent Muslim • .4 percent Jewish
Heterogeneity of Religions in Asian Countries (wikipedia) • China: 67% Taoism/Buddhism, 12% Christian • India: 80% Hindu, 13% Muslim, 2.3% Christian • Japan: 84% no affiliation, Shinto/Buddhists • Pakistan: 97% Muslim • Philippines: 86% Roman Catholics • South Korea: 40% no affiliation, 29% Christian, 27% Buddhists • Vietnam: 85% Buddhists, 8% Roman Catholic/ Christian, 3% Cao Dai
Asian Ethnic Identity Model(Kim, 1981) Ethnic identity is an important concept for understanding how the individual perceives the self in relation to, and adjusts to a predominantly White society, as well as deal with racism. • Ethnic Awareness Stage • White Identification stage • Awakening to Social Political Consciousness stage 4. Redirection stage 5. Incorporation stage
Asian Shared World ViewTe Pou (2010) • Collectivism-needs placed secondary to family and community, shared sense of honor and shame , acceptance on social order, responsibility to follow persons in authority to facilitate pleasant and courteous relationships • Family focus-core, highly involved in life and health decisions, in Indian and South Asian relationships highly structured and formal • Education and wealth focus, many value education and wealth and self-worth define in terms of material and occupational status they achieve, part of duty to family • Importance of “saving face” or not embarrassing family through bad deeds or mental illness • Tolerance of hardship-Asian philosophy put high value in letting things take own course and emphasize life events part of fate, people should learn to accept circumstances • Conflict avoidance and humility-East Asian strong focus on avoiding conflict with others, modesty in communication and in discussing one's achievements • Emotional regulation-East Asian cultures, strong feelings an emotions are avoided, Chinese, Japanese, Korean favor reservation and subtle means of communication, Indians may be more expressive
Asian Shared World View-Influences • Confucianism-ethical system focus on social harmony in 5 relationships: with state, between parent and children, brothers, marital partners, and friends • Taoism-religion based in pre-determination; individuals passive with no control over life, focuses on harmony with nature, and achieving flow and acceptance of one's destiny • Buddhism-suffering is based on desire; loyalty, respect, compassion, and self-control, ancestor worship highly valued • Hindu-belief in karma (one's deeds determine one's destiny in the cycle of birth and rebirth) • Chinese national examination system for government advancement formalized around 600 A.D. Implication is emphasis on education and view that success is more based upon effort versus natural abilities.
Clinical Implications for Asian Shared Values, Beliefs, Behaviors • Holistic attitudes towards health • Asian cultures emphasize interconnectedness and harmony with nature • Chinese medicine views illness as an imbalance between yin and yang and interventions restore balance • Somatization • Mind and body one, thus distress experienced both emotionally and somatically • More culturally appropriate to seek treatment for somatic symptoms • Fatalism • Some Asians may believe that their health conditions are their fate, thus may be more passive in seeking health care • Stigma and shame • Collectivist attitudes thus implication for family and group is emphasized • Belief in predetermination, fate, and karma infers that weaknesses are inherent in person and his/her character
Clinical Implications (continued):Acculturation (Suinn, 2010) • Depression • Associated with marginalization, for males with host culture, for females with culture of origin • Low acculturation associated with more depression • Intergenerational discrepancies in acculturation associated with depression in adolescents • Suicide • Risk factors for adolescents: high parental expectation, issues of shame, intergenerational conflict, perfectionism, and problem-solving deficiency • Counselors/matching • Clients with high Asian values rated Asian-American counselors as more empathic, while more acculturated students evaluated European-Americans as more empathic
Health Disparity: Underutilization of Mental Health Services • Asians 2-5x less likely to seek mental health services than whites • Asians who seek services tend to have more severe mental health problems • More likely to prematurely terminate psychotherapy • (e.g. After initial contact, one third may drop out before initial intake) • Less likely to reveal mental health problems while in therapy
Reasons for Underutilization/Severity at Onset • Great personal stigma and low stigma tolerance • Mental illness a sign of weakness that would bring shame to family • Thus will tolerate more severity of suffering than Westerners • Western treatment is last resort • Many try to work out problems on own or seek informal support or traditional Chinese medicines, or seek medical professionals first • Buddhists tenets indicating suffering is part of human existence and enduring pain is precursor to character development • For many language may be a barrier
Reasons for Early Termination • Not comfortable with self-disclosure and dealing with emotions typical in Western therapies • Many Asian cultures tend to avoid strong emotional displays, thus not comfortable with emotional emphasis • Strong allegiance to family, thus disclosures about family may seem disloyal • Disclosure a sign of personal weakness • Asian client may not be receiving what looking for • Somatic concerns often not addressed • Asian clients not familiar with Western psychotherapy, thus may be look for more directive counselor or more immediate relief • Need for culturally competent providers to deliver treatment with similar worldviews • For many language would be an additional significant barrier
Cultural Adaptations (Sue et al., 2009) • Method of delivery • Attempts to make intervention more culturally consistent, increase credibility of treatment provider, or make treatment more understandable to ethnic minority client • At minimum, therapist should communicate with client in a manner that is culturally acceptable and appropriate • Content • Refers to the discussion of, or dealing with, cultural patterns, immigration, minority status, racism, and cultural background experiences in the intervention • Content increases understandability and credibility of the intervention and demonstrates the pertinence of the intervention to the real life-life problems experienced by clients
Psychotherapy Adaptation and Modification Framework (PAMF)(Hwang, 2009) • Dynamic issues and cultural complexities • Be aware of dynamic sizing (e.g. when to generalize and when to individualize treatments based on client characteristics) • Be aware and address client's multiple identities and group memberships. • Orientation • Orient client to therapy (e.g. establish goals and structure early in treatment, explain biopsychosocial or holistic approach model of disease development) • Cultural beliefs • Focus on psychoeducational aspects of treatment • Understand how cultural beliefs have influenced help-seeking patterns • Find ways to integrate cultural strengths and healing practices
PAMF (continued) • Client-therapist relationship • Therapist should be professional and present selves as authority figures • Client-therapy roles and expectations should be clearly addressed • Join and engage the client by assessing family background and migration history • Therapist cultural self-awareness and self-identity should be thoroughly explored • Cultural differences in expression and communication • Be aware that notion of psychotherapy and talking about one's problems is culturally foreign to Asians whose communication is often more indirect and not emotion focused. • Somatization is a common idiom of distress. • Cultural issue of salience • Be aware of shame and stigma issues that may influence the treatment process • Be aware of and understand life experiences that may be additional stressors or place client at additional risk for mental illness (e.g. acculturative stress, racism, intergenerational family conflict).
Strategies for reducing shame (Tepou, 2010) • Pay respect to the client • Demonstrate acceptance for the client by creating a warm, open, and supportive atmosphere (verbally and non-verbally) • Avoid intense personal questioning in the first session • Focus on practical help that does not place emphasis on the mind (focusing on the mind may prime feelings of stigma or reluctance to engage in therapy) • Normalize the problems by sharing instances where others have been in the same situation (and emphasize that others have recovered)
Strategies (continued) • Reinforce the confidentiality of therapy • Positively reframe circumstance, and providing feedback and compliments are important for dispelling embarrassment and shame, and facilitate continued interaction with therapy • Focus on the problem as an independent concept rather than focusing on aspects of the client as problematic • Provide clients with information about the biological basis of depression and other forms of mental illness
Case Sample • Joe is a 64 year-old Chinese male who was just referred for PTSD treatment by his PCP due to night sweats, insomnia, and nightmares about the Vietnam War where he experienced combat for the majority of time he was there. Onset of his symptoms appeared to coincide with the downsizing at his engineering firm where 5 of his co-workers in his unit were laid off and a switch to a new demanding supervisor about a year ago. Joe has been losing weight and reported increased use of sick days which worries Joe as he does not want to be the next in line for lay offs. Joe is very reluctant to see a mental health specialist and only agreed because his PCP insisted and fears of losing his job.
Discussion Questions • What may be initial impressions on Joe’s case and how may you approach the initial session? • What are some potential salient issues to explore in conceptualizing Joe’s recent onset of PTSD? • What would be some cultural adaptations to consider?
Summary • Clinicians should be aware of the heterogeneity of Asian-Americans (AA) thus avoid the “one size fits all” bias. Familiarizing oneself with the specific ethnicity of the client they are servicing and listening to individual experiences and values are important. • Many AAs are immigrants, thus issues of acculturation for the individual and family are highly salient. Asking about immigration history is a useful tool to build rapport and gain understanding of the client. • Generally, AAs value allegiance to the group versus individualism, family focus with great efforts to avoid shaming the family, conflict avoidance, emotional regulation, and fatalism.
Summary (continued) • Somatization is a common idiom of distress for AAs who have a holistic view of the person and physical illness, and the latter may be a more appropriate manner of communicating distress to avoid stigma. • AAs often do not seek mental health treatment until their distress is severe. Traditional or medical treatments are typical initial interventions and psychiatric illness is highly stigmatizing for the family. • AAs also tend to be early terminators as they are not used to talk therapies and may be especially uncomfortable in revealing things about the family or talking about emotions. AAs may expect more directive approaches or immediate relief. • There are several useful models to adapt therapies to accommodate AA. Clinicians should be familiar with these techniques and implement them appropriately.
Resources • Fujii, D. (Ed.). (2010). The neuropsychology of Asian Americans. New York: Taylor & Francis. (provides background on 11 different cultures) • Hwang, W. C. (2006). The psychotherapy and adaptation and modification framework.: Application to Asian Americans. American Psychologist, 61, 702-715. (describes PAMF) • Kim, E, et al., (2004). Do general treatment guidelines for Asian-American families have applications to specific ethnic groups? The case of culturally competent therapy with Korean Americans. Journal of Marital and Family Therapy, 30, 359-372. (provides guidelines for cultural adaptation) • National Center for PTSD. (2002) PTSD among Asian Americans and Pacific Islander veterans. Retrieved from http://www.ptsd.va.gov/PTSD/professional/videos/emv-ptsdaamvet-hcp.asp(identifies specific issues for PTSD and Asians)
Resources • Te Pou. (2010). Talking therapies of Asian people: Best and promising practice guide for mental health and addiction services. Auckland: Te Pou o te Whakaaro Nui. • www.tepou.co.nz/.../Talking-Therapies/1000599-talking-therapies-for-asian-people.pdf(describes cultural adaptation) • United States Office of Veterans Affairs. Office of Diversity and Inclusion. Asian American and Pacific Islander Program. Retrieved from http://www.diversity.hr.va.gov/spi/programs/aapi.htm • Census Bureau Facts http://www.census.gov/newsroom/releases/archives/facts_for_features_special_editions/cb10-ff07.html
Resources (continued) • Asian American Resource and Fact Sheets from the National Alliance on Mental Illness (NAMI): http://www.nami.org/Template.cfm?Section=Resources&Template=/ContentManagement/ContentDisplay.cfm&ContentID=21026 • The National Asian American Pacific Islander Mental Health Association (NAAPIMHA): http://www.naapimha.org/ • The UC Davis Asian American Center on Disparities Research: http://psychology.ucdavis.edu/aacdr/ • Asian American Psychological Association: https://aapaonline.org/ • The UCLA Asian American Studies Center: http://www.aasc.ucla.edu/
References • Chang, T., & Subramaniam, P. (2006). Asian and Pacific islander American men's help-seeking: Cultural values and beliefs, gender roles, and racial stereotypes. International Journal of Men's Health, 7, 121-136. • Chu, J., & Sue, S. (2001). Asian American mental health: What we know and don't know. Online Readings in Psychology and Culture, Unit 3. Retrieved from http://scholarworks.gvsu.edu/orpc/vol3/iss1/4 • Hwang, W.C. (2009). The formative method for adapting psychotherapy (FMAP): a community-based developmental approach to culturally adapting therapy. Professional Psychology Research and Practice, 40, 369-377. • Kim J. (1981) The process of Asian American identity development from Sue, et al. (1998). Multicultural Counseling Competencies: Individual and Organizational Development. Sage Productions. Thousand Oaks, CA.
References • Le. C. http://www.cnle.net/ • Lin, K. M., & Cheung, F. (1999). Mental health issues for Asian Americans. Psychiatric Services 50, 774-780. • Reeves, T., & Bennett, C. (2004). We the people; Asians in the United States. Washington DC: U. S. Census Bureau. • Sue, S., et al., (2009). The case for cultural competency in psychotherapeutic interventions. Annual Review of Psychology, 60, 525-548. • Suinn, R. (2010). Reviewing acculturation and Asian Americans: How acculturation affects health, adjustment, school achievement, and counseling. Asian American Journal of Psychology, 1, 5-17.