Download
1 / 33
470 likes | 1.9k Views
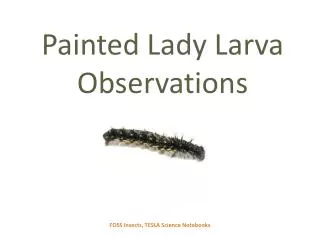
Larva Migrans. 1-Cutaneous Larva Migrans (CLM) 2-Visceral Larva Migrans (VLM) (Toxocaraiasis) Toxocariasis is caused by larvae of Toxocara canis (dog roundworm) and less frequently of T. cati (cat roundworm), two nematode parasites of animals. . Toxocara canis. Toxocara canis.

E N D
Larva Migrans 1-Cutaneous Larva Migrans (CLM) 2-Visceral Larva Migrans (VLM) (Toxocaraiasis) Toxocariasis is caused by larvae of Toxocara canis (dog roundworm) and less frequently of T. cati (cat roundworm), two nematode parasites of animals.
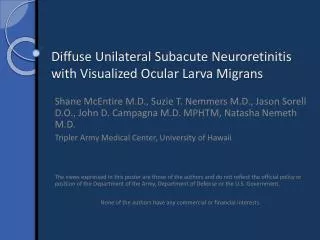
Clinical Features Many human infections are asymptomatic, with only eosinophilia and positive serology. The two main clinical presentations of toxocariasis are visceral larva migrans (VLM) and ocular larva migrans (OLM). In VLM, which occurs mostly in preschool children, the larvae invade multiple tissues (liver, heart, lungs, brain, muscle) and cause various symptoms including fever, anorexia, weight loss, cough, wheezing, rashes, hepatosplenomegaly, and hypereosinophilia. Death can occur rarely, by severe cardiac, pulmonary or neurologic involvement. In OLM, the larvae produce various ophthalmologic lesions, which in some cases have been misdiagnosed as retinoblastoma, resulting in surgical enucleation. OLM often occurs in older children or young adults, with only rare eosinophilia or visceral manifestations.
Laboratory Diagnosis • In this parasitic disease the diagnosis does not rest on identification of the parasite. Since the larvae do not develop into adults in humans, a stool examination would not detect anyToxocaraeggs. • However, the presence ofAscarisandTrichuriseggs in feces, indicating fecal exposure, increases the probability ofToxocarain the tissues. • For both VLM and OLM, a presumptive diagnosis rests on clinical signs, history of exposure to puppies, laboratory findings (including eosinophilia), and the detection of antibodies toToxocara.
Eggs ofToxocara canis. These eggs are passed in dog feces, especially puppies' feces.
Antibody Detection • The currently recommended serologic test for toxocariasis is enzyme immunoassay (EIA) with larval stage antigens extracted from embryonated eggs or released in vitro by cultured infective larvae. • The latter, Toxocaraexcretory-secretory (TES) antigens, are preferable to larval extracts because they are convenient to produce and because an absorption-purification step is not required for obtaining maximum specificity.
Treatment • VLM is treated with antiparasitic drugs, usually in combination with antiinflammatory medications. • The antiparasitic drug recommended in The Medical Letter is albendazole*, with mebendazole* as an alternative.
Causal Agents:Trichinellosis (trichinosis) is caused by nematodes (roundworms) of the genusTrichinella. • In addition to the classical agentT. spiralis (found worldwide in many carnivorous and omnivorous animals), several other species ofTrichinellaare now recognized.
Trichinella spp. • 1- T. pseudospiralis(mammals and birds) worldwide), • 2- T. nativa(Arctic bears) • 3- T. nelsoni(African predators and scavengers) • 4-T. britovi)carnivores of Europe and western Asia).
Geographic Distribution Worldwide. Most common in parts of Europe and the United States.
Clinical Features • Light infections may be asymptomatic. • Intestinal invasion can be accompanied by gastrointestinal symptoms (diarrhea, abdominal pain, vomiting). • Larval migration into muscle tissues (one week after infection) can cause periorbital and facial edema, conjunctivitis, fever, myalgias, splinter hemorrhages, rashes, and blood eosinophilia. • Occasional life-threatening manifestations include myocarditis, central nervous system involvement, and pneumonitis. • Larval encystment in the muscles causes myalgia and weakness, followed by subsidence of symptoms.
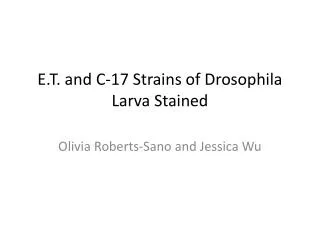
A, B:Encysted larvae ofTrichinellain pressed muscle tissue sample. The coiled larvae can be seen inside the cysts
C, D:Larvae ofTrichinella, freed from their cysts, typically coiled; length: 0.8 to 1 mm.
Laboratory Diagnosis • The suspicion of trichinellosis (trichinosis), based on clinical symptoms and eosinophilia, can be confirmed by specific diagnostic tests, including antibody detection, muscle biopsy, and microscopy.
Antibody Detection Immunodiagnostic tests currently available in the U.S. include enzyme immunoassays (EIA). Antigen preparations may be crude antigens prepared from homogenates ofTrichinella spiralismuscle larvae or excretory-secretory (ES) products produced by cultured larvae.