Download
1 / 17
170 likes | 271 Views
Missouri EMS Central Region September 2012 Webinar Case Review Jeffrey Coughenour, MD, FACS Assistant Professor of Surgery Medical Director, Missouri EMS Central Region. Patient 1. Admission brain CT. Patient 1. Repeat brain CT, 24 hours after admission. Primary Brain Injury.

E N D
Missouri EMS Central RegionSeptember 2012 WebinarCase ReviewJeffrey Coughenour, MD, FACSAssistant Professor of SurgeryMedical Director, Missouri EMS Central Region
Patient 1 Admission brain CT
Patient 1 Repeat brain CT, 24 hours after admission
Primary Brain Injury • Direct result of the disruptive forces that are transmitted during impact • Various mechanism of injury • Result: Several types of mass lesions, axonal shear, skull fracture, etc. • Best therapy—prevention
Secondary Brain Injury • Events after the primary insult that exacerbate injury and worsen outcome • Leading cause of in-hospital death following TBI • Injured brain swelling reduced cerebral blood flow and reduced threshold for cerebral ischemia more damage worsened functional outcome
Secondary Brain Injury • Paramount to therapy is… Avoidance of hypotension and hypoxemia • Intensivist-based management to manage elevated ICP and optimize cerebral blood flow
Evaluation • D “Disability” portion of primary survey • Glasgow Coma Scale score most reproducible measurement of injury • Mild (GCS 14-15): 80% • Moderate (GCS 9-13): 10% • Severe (GCS 3-8): 10% • Report initial GCS, repeat with clinical change • Motor component most predictive of recovery
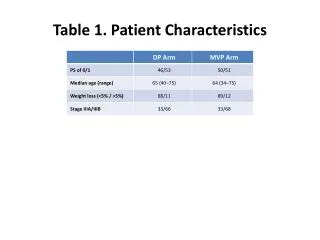
Patient 2 Admission chest radiograph
Patient 2 Left chest
Patient 2 Posterior view
Patient 2 Bilateral sacral fractures
Patient 2 Extravasation from posterior pelvis
Patient 3 Admission chest radiograph
Patient 3 Brainstem hemorrhage
Patient 3 Ischemia/reperfusion injury of the small bowel
Patient 3 Left lower lobar extravasation