Download
1 / 27
280 likes | 776 Views
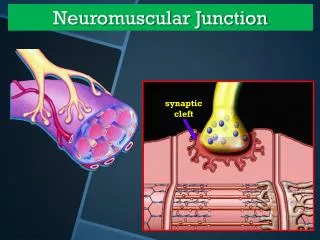
Neuromuscular junction monitoring. Electrodes Stimulation is achieved by passing two electrodes along a nerve and passing a current through them It can be carried out either transcutaneously using surface electrodes or percutaneously wih needle electrodes TYPES A- Surface Electrodes-

E N D
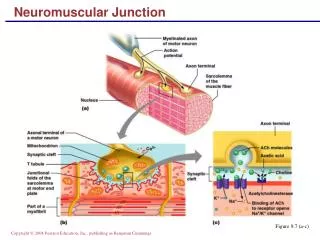
Neuromuscular junction monitoring Electrodes Stimulation is achieved by passing two electrodes along a nerve and passing a current through them It can be carried out either transcutaneously using surface electrodes or percutaneously wih needle electrodes TYPES A- Surface Electrodes- Can be those used for measuring ecg Electrode skin resistance decreases with large conducting area, as do skin burns and pain Large conducting area makes it difficult to obtain supramaximal stimulation Moreover it can stimulate multiple nerves, so it may be better to use pediatric electrodes Skin should be properly cleaned end rubbed with abrasive Electodes for peripheral n. stimulation have different thicknessthan ecg electrodes and have chemical buffers to maintainskin surface ph
METAL ELECTRODES • Two metal plates or balls spaced 1 inch apart,which attach directly to stimulator • --convenient to use • --no good contact • --burns have been reported with their use
NEEDLE ELECTRODES • Useful for providing supramaximal stimulus • --useful when skin is thickened,cold,edematous and in obese, • Also useful in hypothyroid,diabetic and renal failure pts • Other complictions— • Broken needles,infections burns ,nerve damage • There is alo a greater chance of direct muscle stimulation
POLARITY- • Stimulators produce direct current by using one negative and one positive electrodes • Usually positive electrode is red and negative is black • Maximal effect is achieved when negative electrode is placed just over nerve to be stimulated • Positive electrode should be placed along the course of the nerve usually proximally to avoid direct muscle stimulation
METHODS for evaluating evoked responses • A--VISUAL- • Observer should be at an angle of 90 deg. To the motion • Used to count— • No of responses present in TOFstimulus, determine PTC,detect presence of fade with TOFor DBS • POST TETANIC FACILITATION CAN ALSO BE ASSESSED • TOFR is difficult to determine • Visually assessing fade with 100hz tetanic stimulation is fairly accurate for analyzing residual paralysis
B--- TACTILE • Accomplished by placing the evaluators fingertips lightly over ms to be stimulated and feeling the strength of contraction • More sensitive for assessing NMB using TOF. • It can be used to evaluate the presence or absence of responses and/or fade with train of four,double burst,and tetanic stimulation • PTC can be determined • TOFR CAN BE DETERMINED if there is response to all fourstimuli with TOF
Mechanomyography MMG • Utilizes force displacement transducer, such as a strain gauge,attached to fingeror other part of body that can be restrained by a preload and will move when stimulated • The transducer converts the contrctile force into electrical signal,which is amplified and displaced on monitor screen or recorded on chart • Can measure single twitch height,response to tetanic stimulation and TOFR ACCURATELY • Cumbersome, difficult to setup • For accurate results maintenance of muscle temperature within limits is required • Gold standard of scientific measurements of NM system
ACCELEROMYOGRAPHY(ACG,AMG) • Thin piezoelectric transducer is fixed to a moving part. When the part moves voltage is proportional to acceleration of the moving part • Method requires unrestricted movement of the muscle being stimulated • Easy and convenient to use, relative inexpensive and can be interfaced with computer
KINEMYOGRAPHY (KMG) • Utilizes bending sensor placed between thumb and forefinger • Core of sensor is piezoelectric material • Movement is determined by change in the shape of material when it is bent by adductor pollicis muscle contraction • KMG has been compared with MMG except for determining recovery from NMB
PIEZOELECTRIC FILM • Uses disposable piezoelectric film. This is placed so that it spans a movable joint and muscle movement causes the bending of the film which generates voltage which is proportional to the amount of bending • Not as accurate as MMG
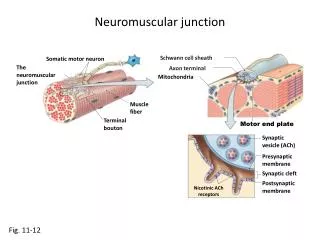
ELECTROMYOGRAPHY(EMG) • Process of recording electrical activity of muscle • When motor n is stimulated , a biphasic action potential is generated in each of the muscle cells it supplies unless some degree of NMB exists. The sum of these action potentials can be sensed by using electrodes placed overmuscle being stimulated • Total 5 electrodes are used • 2 stimulating electrodes on the nerve to be stimulated • 3electrodes –2 receiving ,and one ground are used for recording • Best results are seen when electrodes have been in contact with skin for 15 min before calliberation • Carefull skin preparation helps to give good results
EMG of larynx can also be done • EMG machine automatically determines the supramaximal stimulus, establishes a control response stimulates at selected intervals , measures response and compares it with control . • With nondepolarizing NMB , the action potential amplitude is decreased and there is fade with TOF
Advantages of EMG over MMG • A-less immobilization is required • B-hand or arm need not to be extended or put on board . • C – can be used to monitor laryngeal or diaphragmatic muscles • D– can be used to assess motor nerve blocks induced by regional anaesthesia
Disadvantages— • Sensitive to electrical interference • Response varies according to ms used • Expensive • Response amplitude inc. with dec. temperature • Since site is not immobilized, changes in relative position of recording electrodes cause variation in EMG response
PHONOGRAPHY • Aka acoustic myography • When ms contrcts ,sounds are emitted. These acoustic waves propagate through skin, generating waves which can be recorded by small piezoelectric microphone • Easy to use and can be used on no of different muscles. • Provides stable baseline with little disturbances from artifacts
MONITORING SITES • 1– ULNAR N--- • Most commonly used and adductor pollicis is most commonly monitored • Can be stimulated at elbow , wrist or hand • Wrist– thumb adduction and finger flexion • Elbow– hand adduction + above • Wrist—2 electrodes placed along medial aspect of distal forearm, 2 cm proximal toproximal wrist skin crease with negative electrode distal • Elbow---over sulcus of medial epicondyle of the humerus
EMG monitoring of ulnar nerve • Recording electrodes—hypothenar , thenar , dorsal interosseous ms. For dorsal inter. Ms , active receiving electrode is placed in the web between the index finger and the thumb and the other electrode at the base of second finger • Hypothenar eminence--- both electrodes are placed on palmar side over or the active electrode is placed over hypothenar eminence and the other below the second line on the ring finger or at the base of the dorsum of 5th finger
MEDIAN NERVE— • Wrist-place the electrodes medial to where it would have been for ulnar n • Elbow- adjacent to brachial art. • --stimulation causes thumb adduction TIBIAL NERVE Popliteal fossa—gastroecnemius ms stimulated—causes significant leg movements Sensing electrodes over lateral head of gastroecnemius ms
POSTERIOR TIBIAL NERVE • Electrodes placed behind the medial malleolus and anterior to achillis tendon at the ankle • Stimulation causes plantar flexion of the foot and big toe • Especially useful in children, when it is difficult to find room on the arms; or when hand is inaccessible • There is a lag time with slower onset of relaxation than with ulnar n.
PERONEAL NERVE • electrodes on lateral aspect of of knee • Stimulation causes dorsiflexion of foot FACIAL NERVE Most useful in detecting the onset of relaxation in ms of jaw, larynx ,diaphragm. ACG can be used with facial nerve Negative electrode—ant. To inferior part of ear lobe Positive---just posterior or inferior of the lobe This configuration is more specific corrugated supercilli ms should be observed . With ACG ,the transducer should be placed in the middle of supercilliary arch The facial n should not be used to assess recovery fromNMB becoz responses may show complete recovery while significant NMB is stii present
RECURRENT LARYNGEAL N • Innervates most of the intrinsic ms of larynx • It can be stimulated percutaneously by using two electrodes betweenthe notch between the thyroid and cricoid cartilage • Response can b measured by placing tracheal tube cuff and measuring pressure changes within cuff • EMG in larynx can also be accomplished
USES • Before induction----- • dry ,clean electrodes should be connected to stimulator and placed over selected nerves • Skin should be thoroughly cleaned • Electrodes should be checked to see if the gel is moist • Piece of tape should be placed over electrodes to prevent displacement
INDUCTION • Stimulator can be used to determine-onset time of NMB, detect unusual sensitivity to relaxants and to determine whether the pt is sufficiently relaxed for intubation • Stimulator should be turned on after induction but before giving ms relaxants • Output of stimulator should be inc. until the response does not increase with increasing current, then inc. 10-20%
INTUBATION • Onset of NMB will be faster in centrally located ms like diaphragm, facial , laryngeal and jaw ms than peripheral ms • Monitoring the response of eye ms will reflect the time of onset and level of NMB at airway musculature more closely than monitoring peripheral ms which will underestimate the rate of onset of NMBin airway muscles and may overestimate the degree of block • In majority of pts dissapearence of adductor pollicis response is ass. With good intubating conditions • In EMG monitoring hypothenar eminence may be preferable • Single twitchat 0.1hz is used and clinician wait until the response is barely perceptible before attempting intubation • double burst has been used as an indicator of optimal conditions for tracheal intubation
MAINTAINENCE • During maintenance stimulator can be used to titrate relaxant dosage to the needs of the operative procedure so both over and underdosages are avoided • It is important to correlate the reaction to nerve stimulation with pts clinical condition becoz there may discrepancy between degree of relaxation of the monitored site and that of ms at the site of surgery • TOF is considered the most important pattern for monitoring NMB during anaesthesia • Supramaximal currents are generally used • GOAL– maintain at least one response to TOF stimulation --- no response—further administration of relaxants is not indicated -----2 responses—abd. Relaxation adequate during balanced anaesthesis ---- 3 responses—adequate relaxation if volatile agent is used one twitch is added to above recommendation if facial ms are used
RECOVERY AND REVERSAL Nerve stimulator can detect residual NMB As recovery progresses TOF responses gradually inc. It is best to use a peripheral ms to monitor recovery becoz its complete recovery would indicate residual ms weakness contributing to problems with airway patency are unlikely In past TOFR—0.7 WAS CONSIDERED ADEQUATE Now TOFR-- >90% at adductor pollicis before extubation by MMG IF EMG monitoring is used, residual anaesthetic effects usually prevent the return of T1 to preanaesthetic reference levels ,but TOFR should exceed 90% Residual NMB cannot be reliably detected using TOF if visual/ tactile monitoring is used Detection is somewhat better with TOF
Hazards— • Burns most commonly with needle electrodes • Nerve damage—thumb paraesthesias in MMG due to intramural placement of needle electrodes • Comlications with needle electrodes--- • Pain • Electrical interference