Download
1 / 1
10 likes | 220 Views
Smoking Prevalence and its Association with Surgical Procedures and Co-Morbidities Spring Golden 1 , Hang Saito 2 , Alan Suyama 2 , Elizabeth Tam 1,2 1 John. A. Burns School of Medicine 2 The Queen’s Medical Center. RESULTS. DISCUSSION/CONCLUSIONS

E N D
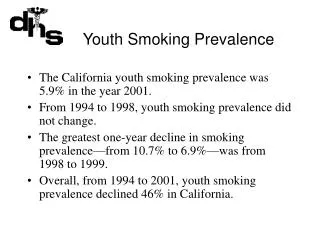
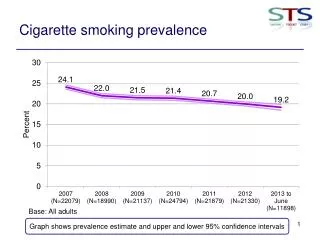
Smoking Prevalence and its Association with Surgical Procedures and Co-Morbidities Spring Golden1, Hang Saito2, Alan Suyama2, Elizabeth Tam1,2 1 John. A. Burns School of Medicine 2 The Queen’s Medical Center RESULTS DISCUSSION/CONCLUSIONS • 16.7% prevalence of current smoking consistent with state smoking rate • Former smokers were older than current or never smokers in this sample. There were no significant differences in sex or BMI between groups. • Any history of smoking was significantly associated with diabetes, consistent with recent reports of a causal association between smoking and glucose intolerance (4) • Knee replacement surgery was the only surgery significantly associated with a history of smoking • This may be due to a confounding effect of age, as people who underwent knee surgery were older and more likely to have been former smokers • There was a tendency to lower rates of smoking or a history of smoking among those scheduled for hysterectomy • Findings are limited by the small sample size, bias toward elective surgeries by a few referring surgeons, and self-report of smoking status or other risk factors • INTRODUCTION • An estimated 17% of Hawaii adults smoke (1) • Smoking increases anesthesia and operative risks (2,3) • Alters vascular functioning, blood coagulation • Alters the cytochrome p450 metabolic enzyme, and other metabolic pathway • Impairs oxygen and vitamin D metabolism • Complete cessation for 8 weeks before surgery significantly reduces incision complications and reduces other complications (2) • Smoking status, therefore, is a necessary to address preoperatively • Anesthesia Pre-Operative Evaluation Center (APEC), Queen’s Medical Center: • Promotes better surgical and anesthesia outcomes through pre-surgical evaluation and education • Patients referred by surgeons complete a Preoperative Anesthesia Health Assessment Questionnaire • APEC nurses follow up with telephone interviews to gain patient histories APEC Smoking Prevalence Demographics and Smoking Status • Previous smokers were older with a mean of 61 years compared to the current smokers and non-smokers (p<0.001) • Data collected for 342 cases • The prevalence of smokers in APEC was determined to be 57/342 (16.7%) NEXT STEPS • Extend the retrospective review to increase sample size of referred patients and referring surgeons • Design focused studies that incorporate objective measure of current smoking (exhaled carbon monoxide, urine cotinine) to understand smoking as a risk factor for other conditions or surgeries • Smoking cessation should be further emphasized in pre-operative evaluation and education and in diabetes prevention and management especially in Hawaii due to the high population of diabetics PURPOSE • Determine prevalence of current and former smokers among patients referred to APEC • Determine if particular types of surgeries and co-morbidities are more strongly associated with current or former smoking Surgical Procedure and Smoking Status Co-morbidities and Smoking Status • REFERENCES • Behavioral Risk Factor Surveillance Survey. Hawaii Smoking Prevalence. Center for Disease Control, 2005. <www.cdc.gov>. • Moller, A. and Tonnesen H. Risk reduction: Perioperative Smoking Intervention. Best Practice Research Clinical Anesthesiology. 2006: 20(2), 237-48. • Moller, A.M. et al. Impact of Lifestyle on Perioperative Smoking Cessation and Postoperative Complication Rate. Preventive Medicine, 2003: 36(6), 704-9. • Willi, C., Bodenmann, P. Ghali, W. Faris, P., and Cornuz, J. Active Smoking and the Risk of Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA. Dec 2007: 298(22):2654-2664. • Barclay, Laurie. Active or Passive Smoking May Be Linked to Glucose. Medscape Medical News, 2006. <www.medscape.com>. METHODS AND MATERIALS • IRB approval obtained from Queen’s Medical Center Review Board • Retrospective review of 364 consecutive APEC telephone interviews May-June 2005 • Variables included the patient’s age, gender, BMI, smoking status, other illnesses, and surgery date • Smoking status classified as current smokers, quit smokers and never smokers • Statistical analysis • Differences between Current, Quit and Never smokers in gender, age, and BMI were determined by 1-way ANOVA test • Associations between co-morbidities or surgical procedures with smoking status were analyzed by Chi-square test and Fisher’s Exact test • A p value ≤ 0.05 was considered significant • Significant association only found between smoking status and knee replacement surgeries (p= 0.045) • Although not significant, there may be an association between hysterectomy surgery and smoking status • Most common surgeries: hip replacement (18 procedures), knee replacement (15 procedures), cholecystecomy (12 procedures), hysterectomy (12 procedures), lumbar fusion (14 procedures) and cervical fusion (12 procedures) • Diabetes was significantly correlated with smoking status (p=0.039) ACKNOWLEDGEMENTS We thank Ms. Caroline Jiang for statistical analysis. This work was supported by: The Queen’s Medical Center Summer Research Scholarship American Lung Association of Hawaii Leahi Fund Tobacco Prevention and Control Trust Fund Hawaii Community Foundation