Download
1 / 30
300 likes | 427 Views
AXIS – Chapter 8. Direction of the current of ventricular depolarization. Depolarization of the heart proceeds down and to the left in the Frontal Plane I + AVF + = Normal Quadrant I+ AVF - = LAD I- AVF - = Extreme LAD I- AVF+ = RAD

E N D
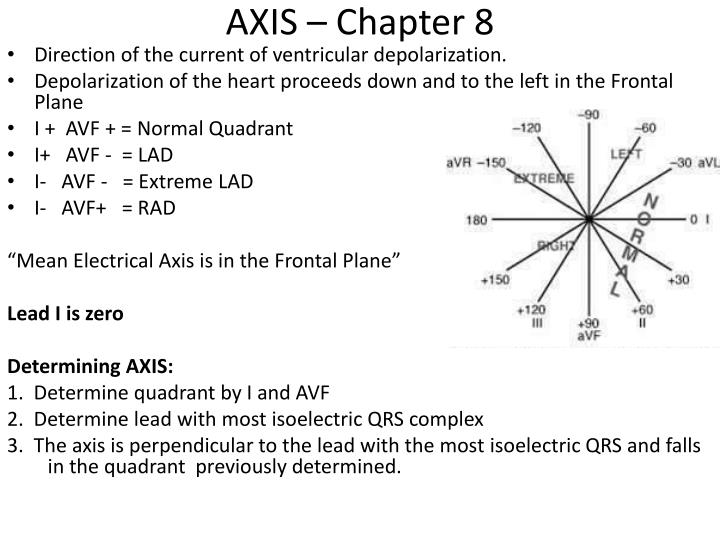
AXIS – Chapter 8 • Direction of the current of ventricular depolarization. • Depolarization of the heart proceeds down and to the left in the Frontal Plane • I + AVF + = Normal Quadrant • I+ AVF - = LAD • I- AVF - = Extreme LAD • I- AVF+ = RAD “Mean Electrical Axis is in the Frontal Plane” Lead I is zero Determining AXIS: 1. Determine quadrant by I and AVF 2. Determine lead with most isoelectric QRS complex 3. The axis is perpendicular to the lead with the most isoelectric QRS and falls in the quadrant previously determined.
I + AVF + = Normal QuadrantAVL is most biphasic (-30 degrees)Normal Axis 60 degrees
I + AVF - = LAD AVR is most biphasic (-150 degrees)LAD -60 degrees
I + AVF + = Normal AVF is most biphasic (90 degrees)Normal Axis 0 degrees
I - AVF + = RAD AVR is most biphasic (-150 degrees)Right Axis Deviation 120 degrees
I and AVF are isoelectricMost of the limb leads are isoelectric, meaning the mean electrical axis of this patient is not in the frontal plane, but traveling perpendicular to the frontal planeIndeterminate Axis
Right Bundle Branch Block • Right bundle branch is “cut”. • May be ischemic or have degenerative changes. • Septum is activated by fibers that originate from the LBB. Depolarization occurs from L to R. • Note normal ECG: R wave for V1 & V2 is small with a large S wave, whereas V5 & V6 has a large R wave and no “s” wave.
RBBB For various reason the classical pattern is not always there. Wide QRS (>0.12 secs) rSR’ in V1 & V2 qRs in V5 & V6 However in all cases the R wave is larger than normal for right chest leads and the QRS is wide.
LBBB • Right BB is normal and LBB is “cut” and will depolarize slowly. Septal activation is also effected. • Net Vector of current is toward the Left Ventricle so there will large R waves in V5 & V6 and Q waves in V1 & V2. • LV slower depolarization = wide QRS in the chest leads. • Pattern: Wide R (maybe notched) wave in V5 & V6 Wide QS in V1 & V2. • Incomplete BBB: > 100 ms <120 ms or 2.5-3.0 boxes
Rate Related (Exercise Induced) BBB • The stress of exercise or high heart rate can cause a BBB due to ischemia or degenerative changes. STOP THE TEST!
Secondary ST-T changes from BBB • LBBB • ST Elevation in V1 • ST Depression/T wave inversion V6 • RBBB • ST Depression/T wave inversion in V1
Intraventricular Conduction Delay Figure 10.6 Above ECG pattern is neither that of a RBBB or a LBBB. QRS is abnormally long (>100 ms or 2.5 boxes) No recognizable characteristics of either block.
Fascicular (Hemi)blocks “failure of one of the fasicles” • Fascicle = bundle of nerve fibers • LBB has 2 • One may function normal and the other may not. • Mild increase in QRS duration but a major axis shift
Left Anterior Fascicular Hemiblock Axis shifts to LEFT. Right posterior functions normally while left anterior fails (?) I+ AVF - = LAD (-60) AVR most isoelectric Criteria: Axis shifts to LEFT. S wave in AVF is deeper than the height of R wave in I The axis is more negative than 45 degrees and there is a Q in aVL = abnormal septal activation.
Left Posterior Fascicular Hemiblock left anterior fascicle of LBB is normal but the posterior fascicle fails. I- AVF+ = RAD (120) AVR is most isoelectric Axis is greater than +120. Rhythm is Afib