Download
1 / 28
280 likes | 483 Views
Chronic Carpal Tunnel in a Landscaper. Jay Hartnett, DPT. Patient Info: John. Age: 28 Occupation: landscaper Chief Complaint: 5-6 year history of pain, numbness & tingling in bilateral forearms & hands (R worse than L). What information about the patient’s symptoms would you like to know?.

E N D
Chronic Carpal Tunnel in a Landscaper Jay Hartnett, DPT
Patient Info: John • Age: 28 • Occupation: landscaper • Chief Complaint: 5-6 year history of pain, numbness & tingling in bilateral forearms & hands (R worse than L)
What information about the patient’s symptoms would you like to know?
Subjective Information • Pain Rating: Best=0/10, Worst=8/10, Current=5/10 • Pain Description: tight & achy in bilateral forearms/wrists; numbness & tingling in hands at night • Symptom Onset: intermittent symptoms since college that recently increased with landscaping work over the last 2 months • Aggravating Activities: gripping, typing, driving, & SLEEPING (pt regularly wakes 2-3x/night secondary to paresthesias in hands) • Relieving Activities: shake out hands, stretch • PMHx: Various injuries during high school & college rugby career: 2-3 stingers (R>L), separated R shoulder, broken R collarbone, wrist fractures, MVA x 2, mother has CTS • Diagnostic Tests / Imaging: none • Previous Treatment: none • Patient Goals: sleep through the night, work, drive & type without pain
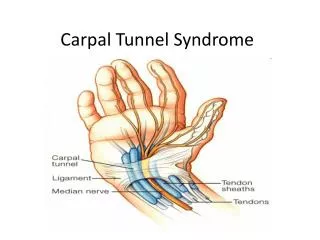
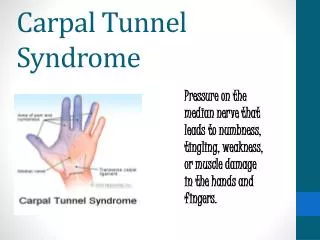
Question 1 What nerve is compressed in Carpal Tunnel Syndrome? • Median • Ulnar • Radial • All of the above
Closer look at Past Medical History • What is a Stinger? • An injury to the brachial plexus, either at the neck or shoulder, that results in often temporary stinging or burning pain that spreads from the shoulder to the hand like an electric shock • John reports he had at least 2 on his L & 1 on his R during Rugby // symptoms always resolved within a day or 2 • Separated Shoulder=AC Joint Separation • Pt reports a grade 2 separation during HS rugby // still gets R shoulder pain with running • Motor Vehicle Accidents: pt denies any injury from either accident • Multiple Wrist Fractures: Compound fracture of distal radius & ulna from falling of monkey bars in kindergarten; Greenstick fractures of both forearms at ages 9 & 10 // pt reports all healed without complications
Question 2 • A greenstick fracture only occurs in infancy or childhood because the bones are not yet fully ossified. • A. True • B. False
What type of objective tests would you like to perform & why?
Objective Information • Posture: forward head & rounded shoulders • Neuro Screen • Myotomes: • C5 (Deltoids): 5/5 • C6 (Biceps): 5/5 • C7 (Triceps): 5/5 • C8 (Thumb Extensors): 5/5 • T1 (Interossei): 5/5 • Dermatomes: intact to light touch C4-T2 • Reflexes: Not Assessed
Objective Cont. • Cervical AROM: full & pain-free • Shoulder & Elbow AROM: full & pain-free bilaterally • Wrist AROM: • Flexion: R=80° L=85° • Extension: R=90° L=85°* pain dorsally • Radial & Ulnar Deviation: full & pain-free • Radio-carpal & Ulnar-carpal Joint Mobility: slightly hypo bilaterally with distraction, posterior & anterior glides • Shoulder Strength: 5/5 bilaterally for FLX, ABD, IR, & ER • Scapular Strength: 4/5 bilaterally for Mid Trap & Low Trap • Grip Strength with hand-held dynamometer: R=104 lbs, L=102 lbs
Objective Cont. Special Tests: • Spurlings: (-) bilaterally • Neural Tension: (+) on R for median bias • Tinel’s & Phalen’s: (+) bilaterally Palpation: TTP & increased tissue tension in bilateral forearm flexors & extensors, palmar fascia, R pectoralis minor, R scalenes, elevated & painful first rib on R Cervical Joint Mobility: WNL
Question 3 • In long-standing Carpal Tunnel Syndrome, which muscles of the hand would you expect to be weak? • A. Abductor pollicis brevis • B. Opponens pollicis • C. Flexor pollicis brevis • D. All of the above
Pertinent Findings • Poor posture • History of cumulative traumas (wrist fractures, stingers, MVA’s, separated shoulder) • Increased reactivity of forearm flexors/extensors • Elevated & reactive 1st rib on R • (+) Median nerve sign on R; Phalen’s & Tinel’s at wrist (+) bilaterally • Genetic link- possible congenitally narrow tunnel
Assessment John presents with abnormal posture, increased of forearm musculature, muscle tightness, neural tension & decreased strength that are contributing to his current pain & functional limitations. • Short Term Goals (3-6 visits): Complete work duties with no greater than 3/10 pain, Type pain-free at the computer for at least 1 hour, Sleep comfortably through the night • Long Term Goals (7-12 visits): Improved postural awareness of optimal chin & scapular position throughout day, Scapular strength=5/5 bilaterally to enable pt to maintain optimal mechanics during work duties, Complete all work duties with no greater than 1/10 pain
Plan of Care Impairment Treatment Soft tissue mobilization Tenderness forearm musculature Etc etc…….
Initial Evaluation Treatment • Postural education, sleep & work modifications • STM to R palmar crease, forearm flexors/extensors • Radiocarpal & ulnocarpal distraction, posterior & anterior glides • Instructed patient on stretches for wrists & pectorals • Ice cup massage R forearm *Instructed patient to thoroughly wash hands & forearms after treatment! **Recommended patient contact physician regarding treatment for poison ivy ***Recommended patient purchase wrist splints to wear at night
Posture Good Bad
Sleeping Position Suggested modification Prior position
Pushups Modified Standard
1st Follow-up Visit: Subjective • Pain: current=2/10 wrist flexors & extensors- feel tight from work • Has not woke up with symptoms since purchasing wrist splints • Completed a Medrol dose pack- poison ivy much better • Stretching frequently throughout day • Not moving as heavy loads with wheelbarrow at work & using better mechanics as keyboard
Question 4 • What type of drug is a Medrol dose pack? • Analgesic • Antihistamine • Steroid anti-inflammatory drug • Non-steroid anti-inflammatory drug ( NSAID)
Interventions • Review posture • STM to bilateral scalenes (increased tenderness on R) • 1st rib mobs on R • R Pec minor STM • Median nerve glides on R • STM to palmar fascia, forearm flexors & extensors • General wrist mobs for distraction, posterior & anterior glides • Wrist flexion & extension stretches • Mid Trap & Low Trap strengthening • Ice cup massage to bilateral forearms
Re-evaluation at 5th Follow-up Visit (9/16) John rates overall improvement at 85% since Initial Evaluation (8/27) • Better postural awareness & improved ergonomics at home & work • No pain the last 2 days of work except occasional shooting pain into R hand when picking up heavy objects • Can now work at computer without any pain or limitation • Driving is no longer an issue • Getting back into workout routine & even planning on starting yoga • Now sleeping comfortably throughout the night with braces
At Revaluation (5th visit 9/16) • Improving soft tissue mobility of tight musculature from IE • First rib mobility on R improving • Decreased reactivity of R median nerve • Mid Trap MMT: 4+/5 bilaterally • Low Trap MMT: 4+/5 bilaterally • Grip Strength with HHD: R=103 lbs, L=114 lbs (at 8/27: R=104 lbs, L=102lbs) • Phalen’s: (+) bilaterally • Tinel’s & Median nerve bias (-) bilaterally
Outcomes / Results • I am currently still treating this patient. • Any comments or recommendations?