Download
1 / 31
330 likes | 533 Views
MANAGING GLAUCOMA IN AFRICAN CONTEXT. Pr Amel Ouertani Chairman of Ophthalmology Department- Charles Nicolle University Hospital-Tunis Vice-President Middle East African Council of Ophthalmology MEACO Secretary General Middle East African Glaucoma Society ,MEAG’S

E N D
MANAGING GLAUCOMA IN AFRICAN CONTEXT Pr Amel Ouertani Chairman of Ophthalmology Department- Charles Nicolle University Hospital-Tunis Vice-President Middle East African Council of Ophthalmology MEACO Secretary General Middle East African Glaucoma Society ,MEAG’S Secretary General Nadi Al Bassar GA- IAPB, September17-20-hydrabad
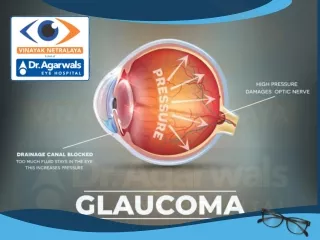
INTRODUCTION WHO: Glaucoma is the 2nd cause of visual impairment & blindness in both the developed and developing world
INTRODUCTION Global Prevalence of glaucoma 1990 WHO program for prevention of blindness
Causes Of World Blindness Avoidable • Trachoma • Onchocerciasis • Corneal opacities Avoidable/Treatable • Cataract • Congen. Cataract & Glaucoma Still difficult to manage +++ • Glaucome • D. Retinopathies
Magnitute of Glaucoma in Africa • ♦POAG • In most populations OAG rates: 1% to 4% • African-derived pop°: rates of 8% to 9%. • Black race : Risk factor for POAG ♦ PCAG:0.5% (recentsurveys in Africa)
Prevalence Of Chronic Glaucoma Tanzania, Africa & rest of the world In general, steady increase after Age 40 Often earlier in dark skinned people!
COAG: Worldwide Distribution (WHO 1990 Estimates) POPULAT. 1.2 bil 0.7 bil 1.2 bil When compared to other regions, COAG is proportionately worse in Africa
Glaucoma differ in Africa from elsewhere by its clinical presentation, agressiveness, resistance to treatment LATE DIAGNOSIS and thus bad prognosis
Glaucoma Challenges in Africa • Adequate Infrastructure for early detection, diagnosis, treatment and follow up of COAG • Treatment options for the management of COAG • Availability and affordability of anti-glaucomatous medicines • Availability of skilled personnel in the country, trained for Glaucoma surgery • Patients continuous education • Establish National Glaucoma guidelines/policies
Challenges related to early Detection and Diagnosis ♦ Glaucoma is a silent disease, with very few signs or symptoms, until in advanced stages ♦ Loss of vision is slow & progressive, & hardly perceptible: ♦ Diagnosis is difficult especially in early cases, as no one test is sufficient at that stage to diagnose ♦ As a resultmany patients present late to the clinic (29% of Gl. patients & 53%of Gl. Eyes already blind!)
Whatisneeded ♦Diagnosis at a stage where patients still have some usefull vision
►HOW ??? ♦ Community/pop based screening program ?? ♦ Opportunistic screening ?? ♦ Identify an inexpensive practical and valid screening test acceptable by population Surveys?? RAAB?? ♦ Agreement on whom to screen and whom to treat
Infrastructure related Challenges Current Situation What is needed ♦ Ensure - all training institutions, - most (if not all) tertiary eye units, as well as- all high volume eye units are fully equipped to manage Glaucoma ♦ For each group, set priorities & a realistic timeframe to achieve it ♦ Still very few eye units fully equipped to assess & confirm glaucoma Dg ♦ Still many tertiary units without even functional visual field equipment ♦ Many rural patients are still beyond reach
Challenges related to Treatment Options Medical Treatment ♦ Easy , less threatening ♦Rare in most parts of many countries, with entire provinces with no place to buy any ♦ Very expensive, even to those with a regular source of income ♦ hardly sustainable. :Available & affordable only in NGO/Mission supported structures ♦ Compliance :Poor • Failure Rate is HIGH ► NOT SUCH A GOOD OPTION IN AFRICA
What is needed A national policy framework that could include: ♦a national strategy for the procurement and distribution of anti-glaucoma drugs, ♦ a simple but workable system to identify & subsidize poor Patients ♦ Partners willing to support such a system in the long term
Challenges related to Treatment Options Laser Treatment ♦ Easy, satisfactory for patient and doctor ►laser needed ►Efficacywears off
Challenges related to Surgery Options Current Situation ♦More difficult,not easily accepted □In early stages Because it hardly results in “improved vision” □ In advanced cases :additional challenge is Having to perform surgery on the only good eye ♦ Still too few well trained and confident glaucoma surgeons ►Yet because it is a “one time” type of TT , costs less and requires less follow up, itisoften the only realistic option to many
What is needed Patient education Given the current shortage, acceptable strategies to increase the nb of glaucoma surgeons in each country must developed & implemented This may require the retraining of many existing surgeons
Challenges related to Limited Skilled Personnel Current Situation What is needed ♦ Update the list of skilled personnel in each country ♦ Identify & support all existing personnel (especially cataract surgeons) needing re-training (+ equipment). ♦ Identify & support training institutions needing subspecialty training ♦Fully trained Gl specialists still too few in many countries, non existent in some ♦ Not all cat surgeons equally Well trained in glaucoma surgery ♦ In many countries, entire regions Still with no one skilled in clinical& surgical management of gl. ♦ Many (of the few) well trained still operate with less than the min equipt
Challenges related to patients’ ignorance of the disease Current Situation What is needed First : ensure patients targeted for health education will have easy access to functional glaucoma services and affordable drugs if needed Develop a culturally sensitive IEC strategy for glaucoma nation-wide Target patients at risk • Knowledge about glaucoma is limited • Because glaucoma is asymptomatic means many patients are likely to report late • At the same time, patient’s education is of little help where back up services either don’t exist or are not operational
Steps for challengingglaucoma for the next 10 years ♦ Advocacy: Glaucoma : Public health problem ♦ Include glaucoma in national plans for POB ♦ Collection of Epidemiological data at the country and the continent level ♦ Evaluation of the magnitude of the problem: Surveys?? RAAB??
Contribution of governments++ National Politicalcommitment ♦ Repair and develop health systems (with the help of regional structures such as AU/NEDAP, and with WHO’s technical support.) ♦ Train and retain an additional 1 million health workers by 2015 ♦ Increase annual budgets to health ♦ Improve procurement systems (including greater availibility of pricing information and reference to regularly updated essentiel drug list) can have a valuable impact. Abolish user fees, as recomended to governments by the commision for Africa
Supranational and International Organizations ◘WHO ◘ PBU ◘ MEACO ◘ ICO ◘ AAO
Communityinvolvment:NGO+++ NADI AL BASSAR CATARACT CAMPAINS
International Aid 1°/ Africacan’taffordhighprice of medicine. ▪ (WTO) TRIPS agreement contains important flexibilitiesthatcanbeused to accessmedicines (likecompulsory licence allowing local production of patent protectedmedicines) ▪ Pharmaceutical compagnies can support by developingdifferentialpricingoffers for antiglaucomadrugs, ▪ 2°/ Equipments
The need for National Glaucoma Guidelines/Policies • Many of the challenges discussed in this presentation could and should be addressed through such guidelines • For many countries this would require at least 2 actions:- update the glaucoma strategy section in their existing national plans- set up an HRD sub-group to oversee the development and implementation of the guidelines • In most countries, making anti-glaucoma drugs widely available & affordable will require the development and enforcement of national policies
CONCLUSION Much of what is needed is to start addressing the many challenges of Glaucoma Yet, glaucoma patients across Africa are still among the least served of all eye care patients What is needed now is concrete action and sustained support, even in small steps.
Challenges related to Treatment Options Surgical Treatment ♦ More difficult, and not Easily accepted by most Patient