Download
1 / 58
600 likes | 1.01k Views
IUI, Ovarian Stimulation and Complications. G. I. Serour , FRCOG, FRCS, FACOG (hon) Professor of Obstetrics and Gynaecology Director, International Islamic Center for Population Studies and Research , Al-Azhar University Clinical Director, The Egyptian IVF-ET Center, Maadi, Cairo, Egypt

E N D
IUI, Ovarian Stimulation and Complications G. I. Serour, FRCOG, FRCS, FACOG (hon) Professor of Obstetrics and Gynaecology Director, International Islamic Center for Population Studies and Research , Al-Azhar University Clinical Director, The Egyptian IVF-ET Center, Maadi, Cairo, Egypt FIGO President ERC/ELG March 3rd-4th, 2012
Items Addressed • What is IUI. • Indications. • Effectiveness. • Cost Effectiveness. • Factors affecting success rate. • Advantages and complications.
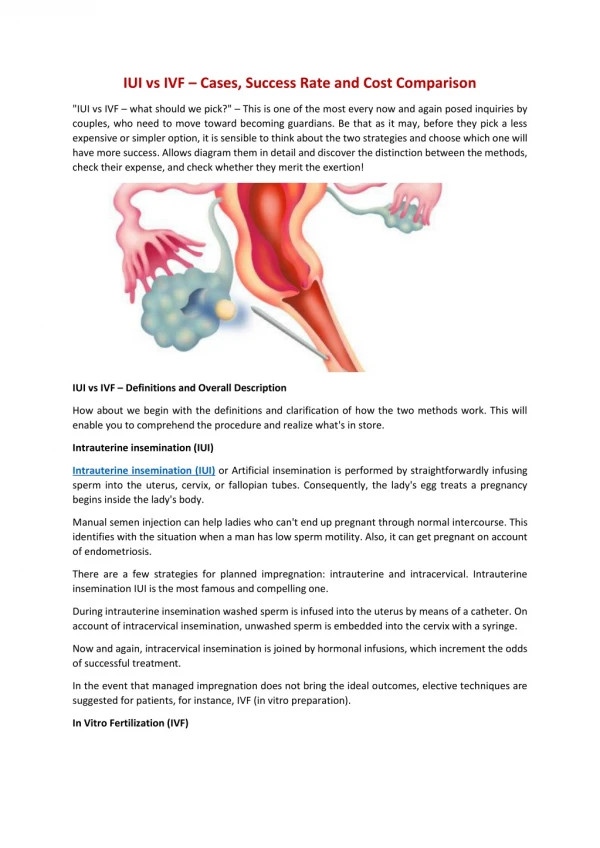
The rationale behind intrauterine insemination (IUI) with homologous sperm is bypassing the cervical-mucus barrier and increasing the number of motile spermatozoa with a high proportion of normal forms at the site of fertilization.
This interest in IUI is undoubtedly associated with the refinement of techniques for the preparation of washed motile spermatozoa.
Semen Preparation Techniques • Swim up. • Albumin • Percoll • Minipercoll • Glass wool filtration • Sephadex separation • Migration sedimentation • Glass blood separation
The washing procedures are necessary to remove prostaglandins, infectious agents, antigenic proteins, non-motile spermatozoa, leucocytes and immature germ cells.
This may enhance sperm quality by decreasing the formation of free oxygen radicals after sperm preparation. The final result is an improved fertilizing capacity of the sperm in vitro and in vivo. Aitken RJ, Clarkson JS et al. Reprod Fertil 1987;81:459-469
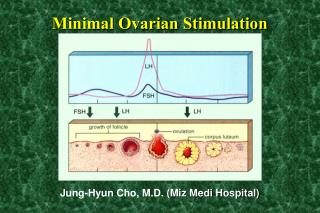
Patient preparation Natural cycle MOH - CC – hCG -CC – hMG –hCG -rec FSH – hCG -GnRH-hMG (rec. FSH) - hCG
Timing of IUI Basal Body Temperature LH Surge ( urine/serum) US
Sample for IUI Fresh semen Split ejaculate Different volumes Washed semen +/- - Antioxidants - Platelet Activity Factor - Follicular Fluid.
Sites of insemination Intrauterine (IUI) Intracervical (ICI) Intraperitoneal (IPI) Cap insemination Trans cervical / intrafallopian (ITI)
Since IUI programmes are easy to run Cheap and do not need sophisticated equipment IUI is an attractive choice for the treatment of some infertility cases in resource poor countries.
It is generally accepted that intrauterine insemination (IUI) should be preferred to more invasive and expensive techniques of assisted reproduction and be offered as a first-choice treatment in some cases of subfertility. Ombelet W. et al. hum Reprod, 2008 , doi:10.1093/humrep/den165
Indications Male factor subfertility Unexplained infertility Endometriosis. Combined ovulatory and ♂ factor infertility. Cervical and immunological infertility Sexual dysfunction infertility.
Male Factor Subfertility In long standing infertility caused by reduced sperm quality expectant treatment seems to be disappointing with a spontaneous conception rate of only 2% per cycle. Collins J A et al. Fertil Steril; 1995, 64:22-28
The lower reference limit for semen analysis WHO Lab Manual of Human Semen 2010
Male factor Infertility (OAT) • Oligozoospermia (O) • Asthenozoospermia (A) • Tratozoospermia (T)
Male subfertility In male subfertility IUI with or without COH a pregnancy rate of 10-18% per cycle has been reported. -Stone BA et al 1999. Am. J Obstet Gynecol, 180:1522-1534 - Ombelet W et al 1995,Hum. Reprod. 10 (Suppl. 1):90-120 - Ombelet W et al 1997. Hum. Reprod. 12:1458-1463
Male subfertility A Cochrane review showed that IUI is superior to TI, both in natural and in cycles with CoH. Cohlen BJ et al 2000. (Cochrane Review) Cochrane library, issue 4, update software, Oxford.
IUI in natural cycles should be the treatment of choice in case of male subertility, providing an insemination motile count (IMC) of more than 1 million can be obtained after sperm preparation and in the absence of a triple sperm defect ( according to WHO criteria) . Cohlen BJ et al 2000. (Cochrane Review) Cochrane library, issue 4, update software, Oxford.
IMC and sperm morphology are the most valuable sperm parameters to predict IUI outcome in male subfertility. • Ombelet W et al 2003. Reprod Biomed Online 2003;7:485-492 • Duran EH et al , 2002. Systematic Review. Hum. Reprod Update ;8:373-384
There is a trend towards increasing conception rates with increasing IMC, but the cut-off value above which IUI seems to be successful, however varies between 0.3 and 20X106 . • Ombelet W et al 2008. Hum. Reprod. Doi:10.1093/humrep/den165
In cases with < 1 million motile spermatozoa, IUI remains successful provided the sperm morphology score using strict criteria is 4% or more (cumulative ongoing PR of 21.9% after three IUI cycles). • Centole GM 1997. J. Androl; 18:448-453
A cut off level of: 0.8 million motile spermatozoa after washing . Metaanalysis(Van Weert et al 2004 ) 30-50% Total sperm motility before sperm preparation ( OmbeletW et al 1996 Dickey et al 1999, Montanaro et al 2001, Lee et al, 2002)
Infertility work -up HSG, Laparoscopy, HSCS.. No tubal factor Washing procedure IMC< 1 million IMC> 1 million IMC< 1 million Morphology <5% IUI 4x IVF < 30 % or no fertilization ICSI Proposed algorithm of male subfertility treatment at the Genk Institute for fertility Technology (ICM, insemination motile count of the number of motile spermatozoa after washing procedure; HSG, hysterisalpingography; HSCS, hysatero-salpingo-contrast-sonography) Ombelet W et al 2008). ESHRE Monograph , 1: 64-72
Unexplained infertility Meta –analysis comparing IUI and TI in natural cycles showed no difference in results; therefore, IUI in natural cycles seems ineffective in case of unexplained infertility. Cohen BJ. Gyn. Obst. Invest; 2005,59:3-13
When controlled ovarian hyperstimulation (COH) is used, IUI becomes effective compared with TI Cohlen BJ. Gyn. Obst. Invest ;2005;59:3-13
There is evidence that IUI with COH increases the live birth rate compared with IUI alone. The likelihood of pregnancy was also increased for treatment with IUI compared with TI in stimulated cycles. Verhulst SM et al. Cochrane Database Syst Rev 2006;18::CD001838
Cervical Factor Infertility The results of a meta-analysis of randomized controlled trials comparing IUI with timed intercourse (TI) for couples with cervical factor infertility showed a significant improved probability of conception for IUI. Cohlen BJ. Gyn. Obst. Invest ;2005;59:3-13
Sexual Dysfunction infertility Retrograde ejaculation Vaginismus Hypospadius Impotence Infrequent Intercourse during fertile period.
Effectiveness Controversy still surrounds the effectiveness of this very popular treatment procedure.
ESHRE Capri Workshop Group • Stimulated IUI is ineffective in male infertility and the effect on other diagnoses is small. • IUI+CC PR 7% /cycle • IUI+ FSH PR 12 %/ cycle • IUI+FSH MP 13 % • Prevention of premature LH | not a major • Luteal phase support | requirement Crosignani PG et al Hum Reprod Update, 2009, vol 15 No. 3, 265-277
Pregnancy rate per cycle and number needed to treat (NNT)per cycle *Pregnancy rate per cycle is from Reindollar et al. (2007). NNT is from Deaton et al. (1990) before crossover.
ESHRE Capri Workshop Group IUI in stimulated cycles may be considered while waiting for IVF or when in women with patent tubes IVF is not affordable. ESHRE - Hum Reprod. Update, 2009 Vol,15, No. 3, 265-277
In most of these indications, IUI or stimulated ovary/IUI is empiric treatment since it is likely that the majority of infertility involves factors that are untreatable or unknown. ESHRE- Hum Reprod. Update, 2009 Vol,15, No. 3, 265-277
Most studies are retrospective. Studies vary in: - Comparison of study groups. - Use or non use of MOH. - No of inseminations/treatment cycle. - Different sites of insemination. -Various methods of sperm preparation. - Use/non use of additives as antioxidants, platelet activation factor (PAF)…etc
Efficacy of IUI Intercourse in natural cycle IUI in natural cycle Intercourse in stimulated cycle IUI in stimulated cycle Four comparisons to be performed in RCT to (dis) prove the efficacy of IUI with or without MOH Cohen BJ and Tournaye H in Macklon NS et al (ed) informa healthcare 2008
IUI / Other modalities Success rate Singleton live birth rate Cost-benefit analysis Complication rate Invasiveness of the technique Patient compliancy Healthcare cost
Unexplained and moderate ♂ factor subfertility Effectivity has been documented in controlled studies under the condition that the inseminating motile count exceeds more than 1 million motile spermatozoa. Ombelet W. et al. Hum Reprod, 2008 , doi:10.1093/humrep/den165
A comparable cumulative ongoing PR after three IUI cycles for all couples, providing the IMC was more than 1 million was obtained. • Ombelet W et al 1997. Hum. Reprod. 12:1458-1463
Cost effectiveness Published data comparing cost of IVF versus IUI indicate that initiating treatment with IUI appeared to be more cost-effective than IVF in most cases of unexplained and moderate male subfertility - Ombelet W. et al 2003. Reprod Biomed Online; 7:485-492 - Ombelet W. et al 2005. Hum. Reprod. Update ; 11:3-14
In a systematic Review Garceau et al (2002) showed that initially treatment with IUI appears to be more cost-effective than IVF in most cases of unexplained and moderate male subfertility. Carceau L et al 2002. Hum Reprod; 17:3090-3109
IUI versus IVF IVF baby IUI baby 43,000 $ 10,000 $ Van Voorhis et al. Fert. Steril 1998 IVF baby IUI baby 13,000 $ 5,000 $ Goverde et al. Lancet 2000 IUI baby IVF baby 9,500 $ 16,000 $ Philips et al. Hum Reprod 2000
IUI baby 1,500 $ IVF baby 5,000 $ Int J Gynaecol Obstet. 1991 Sep;36(1):49-53
Factors affecting IUI success Age of the female. Natural cycle versus MOH Number of inseminations Number of IUI treatment cycles. Site of insemination Exact timing of IUI Factors affecting embryos implantation Laboratory factors
Live birth rates could not be assessed Anti –oestrogens versus gonadotrophins combined with intrauterine insemination outcome: pregnancy rate per couple. (Contineau AE et al, 2007)
One intrauterine insemination (IUI) versus double IUI in stimulated cycles. Outcome: pregnancy rate per couple. (Contineau AE et al, 2003)
Embryo Implantation Endometrial thickness/polyps Catheter used Us of aspirin and luteal phase support
Uterine Polypi Polypectomy can improve fertility in subfertile women with asymptomatic endometrial polyps. Kuohung W & Hornstein M 2010. Up T o Date . www.uptodate.com
Number and percentage of pregnancies after hysteroscopic polypectomy (n=204) (RCT) 4xIUI Perez –Medina T et al, 2005. Hum Reprod. 20:1632-1635