Download
1 / 1
10 likes | 110 Views
New York State Department of Health: Mandatory Reporting of Clostridium difficile via National Healthcare Safety Network LabID Event – Evaluating the Validity of the Proxy Measure vs. Infection Surveillance. New York State Dept. of Health, Hospital Acquired Infection Reporting.

E N D
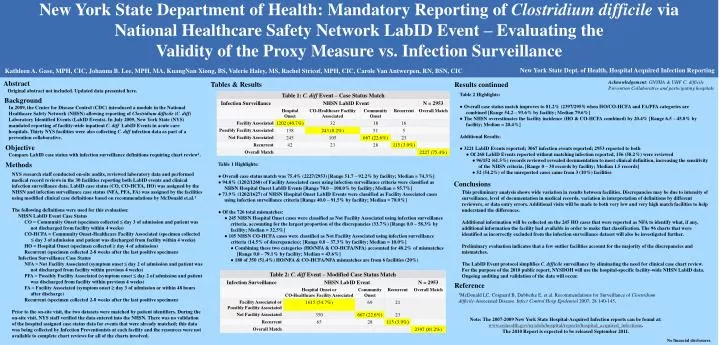
New York State Department of Health: Mandatory Reporting of Clostridium difficile via National Healthcare Safety Network LabID Event – Evaluating the Validity of the Proxy Measure vs. Infection Surveillance New York State Dept. of Health, Hospital Acquired Infection Reporting Kathleen A. Gase, MPH, CIC, Johanna B. Lee, MPH, MA, KuangNan Xiong, BS, Valerie Haley, MS, Rachel Stricof, MPH, CIC, Carole Van Antwerpen, RN, BSN, CIC Abstract Acknowledgement: GNYHA & UHF C. difficile Prevention Collaborative and participating hospitals Tables & Results Results continued Original abstract not included. Updated data presented here. Table 2 Highlights: ● Overall case status match improves to 81.2% (2397/2953) when HO/CO-HCFA and FA/PFA categories are combined [Range 54.2 – 93.6% by facility; Median 79.6%] ● The NHSN overestimates the facility incidence (HO & CO-HCFA combined) by 20.4% [Range 6.5 – 45.8% by facility; Median = 20.4%] Additional Results: ● 3221 LabID Events reported; 3067 infection events reported; 2953 reported to both ● Of 268 LabID Events reported without matching infection reported, 156 (58.2%) were reviewed ● 96/152 (61.5%) records reviewed revealed documentation to meet clinical definition, increasing the sensitivity of the NHSN criteria. [Range 0 – 30 records by facility; Median 1.5 records] ● 52 (54.2%) of the unreported cases came from 3 (10%) facilities Background In 2009, the Center for Disease Control (CDC) introduced a module in the National Healthcare Safety Network (NHSN) allowing reporting of Clostridium difficile (C. diff) Laboratory Identified Events (LabID Events). In July 2009, New York State (NYS) mandated reporting of facility-wide inpatient C. diff LabID Events in acute care hospitals. Thirty NYS facilities were also collecting C. diff infection data as part of a prevention collaborative. Objective Compare LabID case status with infection surveillance definitions requiring chart review1. Methods Table 1 Highlights: ● Overall case status match was 75.4% (2227/2953) [Range 51.7 – 92.2% by facility; Median = 74.3%] ● 94.8% (1202/1268) of Facility Associated cases using infection surveillance criteria were classified as NHSN Hospital Onset LabID Events [Range 70.0 – 100.0% by facility; Median = 95.7%] ● 73.9% (1202/1627) of NHSN Hospital Onset LabID Events were classified as Facility Associated cases using infection surveillance criteria [Range 40.0 – 91.5% by facility; Median = 78.0%] ● Of the 726 total mismatches: ●245 NHSN Hospital Onset cases were classified as Not Facility Associated using infection surveillance criteria, accounting for the largest proportion of the discrepancies (33.7%) [Range 0.0 – 58.3% by facility; Median = 32.5%] ● 105 NHSN CO-HCFA cases were classified as Not Facility Associated using infection surveillance criteria (14.5% of discrepancies); [Range 0.0 – 37.3% by facility; Median = 10.0%] ● Combining these two categories (HO/NFA & CO-HCFA/NFA) accounted for 48.2% of mismatches [Range 0.0 – 79.1% by facility; Median = 43.6%] ● 180 of 350 (51.4%) HO/NFA & CO-HCFA/NFA mismatches are from 6 facilities (20%) NYS research staff conducted on-site audits, reviewed laboratory data and performed medical record reviews in the 30 facilities reporting both LabID events and clinical infection surveillance data. LabID case status (CO, CO-HCFA, HO) was assigned by the NHSN and infection surveillance case status (NFA, PFA, FA) was assigned by the facilities using modified clinical case definitions based on recommendations by McDonald et.al.1 The following definitions were used for this evaluation: NHSN LabID Event Case Status CO = Community Onset (specimen collected ≤ day 3 of admission and patient was not discharged from facility within 4 weeks) CO-HCFA = Community Onset-Healthcare Facility Associated (specimen collected ≤ day 3 of admission and patient was discharged from facility within 4 weeks) HO = Hospital Onset (specimen collected ≥ day 4 of admission) Recurrent (specimen collected 2-8 weeks after the last positive specimen) Infection Surveillance Case Status NFA = Not Facility Associated (symptom onset ≤ day 2 of admission and patient was not discharged from facility within previous 4 weeks) PFA = Possibly Facility Associated (symptom onset ≤ day 2 of admission and patient was discharged from facility within previous 4 weeks) FA = Facility Associated (symptom onset ≥ day 3 of admission or within 48 hours after discharge) Recurrent (specimen collected 2-8 weeks after the last positive specimen) Prior to the on-site visit, the two datasets were matched by patient identifiers. During the on-site visit, NYS staff verified the data entered into the NHSN. There was no validation of the hospital assigned case status data for events that were already matched; this data was being collected by Infection Preventionists at each facility and the resources were not available to complete chart reviews for all of the charts involved. Conclusions This preliminary analysis shows wide variation in results between facilities. Discrepancies may be due to intensity of surveillance, level of documentation in medical records, variation in interpretation of definitions by different reviewers, or data entry errors. Additional visits will be made to both very low and very high match facilities to help understand the differences. Additional information will be collected on the 245 HO cases that were reported as NFA to identify what, if any, additional information the facility had available in order to make that classification. The 96 charts that were identified as incorrectly excluded from the infection surveillance dataset will also be investigated further. Preliminary evaluation indicates that a few outlier facilities account for the majority of the discrepancies and mismatches. The LabID Event protocol simplifies C. difficile surveillance by eliminating the need for clinical case chart review. For the purpose of the 2010 public report, NYSDOH will use the hospital-specific facility-wide NHSN LabID data. Ongoing auditing and validation of the data will occur. Reference 1McDonald LC, Coignard B, Dubberke E, et al. Recommendations for Surveillance of Clostridium difficile-Associated Disease. Infect Control Hosp Epidemiol 2007; 28:140-145. Note: The 2007-2009 New York State Hospital-Acquired Infection reports can be found at: www.nyhealth.gov/nysdoh/hospital/reports/hospital_acquired_infections. The 2010 Report is expected to be released September 2011. No financial disclosures.



















