Download
1 / 37
390 likes | 910 Views
Rheumatic fever. DR : Gehan Mohammed. Learning objectives. Understand the pathogenesis of rheumatic fever. Discuss the Effects of Rheumatic Fever on the three layers of Heart( endocardium,myocardium,pericardium ).

E N D
Rheumatic fever DR : Gehan Mohammed
Learning objectives • Understand the pathogenesis of rheumatic fever. • Discuss the Effects of Rheumatic Fever on the three layers of Heart(endocardium,myocardium,pericardium). • Identify the organs other than the heart that are affected by rheumatic fever. • List the major and minor criteria needed for diagnosis of rheumatic fever. Differentiate rheumatic endocarditis from other causes of endocarditis(Nonbacterial Thrombotic EndocarditisNBTE,Infective Endocarditis)
ACUTE Rheumatic Fever (ARF) • Definition: is an acute, immunologically mediated, multi-system inflammatory disease that follows, after a few weeks of an episode of group A-beta hemolytic streptococcal infection with cardiac and extra cardiac manifestations. • It is characterized by inflammatory reaction involving heart 60% of patients affected by RF, joints in 75% , central nervous system in 10 % and skin in 2%.
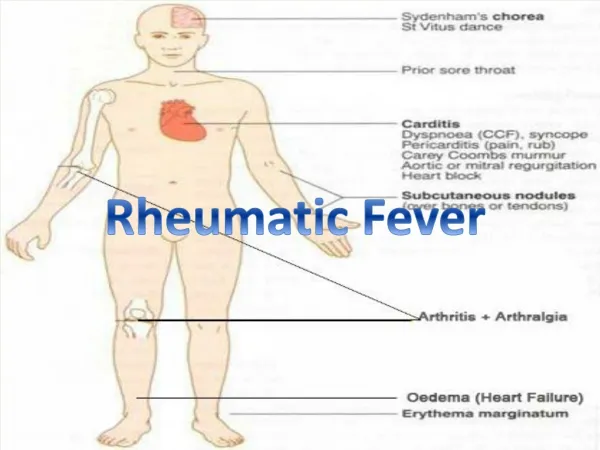
Acute Rheumatic Fever: Clinical • Occurs 10 days to 6 weeks after pharyngitis caused by strept infection so anti streptolysin O (ASO) titer will be high. • Peak incidence: in children 5-15 years. • Acute carditis: pericardial friction rubs, weak heart sounds, tachycardia and arrhythmias. • Extracardiac: fever, migratory polyarthritis of large joints, arthralgia, skin lesions, chorea
Pathogenesis • The causative organisms result in the formation of antibodies. Then These antibodies cross react with joints and the heart which may be due to antigenic similarity between streptococcus and heart tissue. • Immunologic mechanism is the most likely method of damage to the heart .
For diagnosis of rheumatic fever need 2 major or 1 major and 2 minor criteria Johnes Major criteria of rheumatic fever • 1- Carditis • 2- Migrating Polyarthritis affect large joints as knee,ankle which show redness, swollen,hot. Inflamed joints , self limited, become normal within 1-3 days even without treatments so no chronic deformities. • 3- Sydenhem’s chorea : a characteristic series of rapid movements of the face and arms. This occurs late in the disease
For diagnosis of rheumatic fever need 2 major or 1 major and 2 minor criteria Major criteria of rheumatic fever • 4- Erythema margination:common on trunk ,limbs ,not pruritic. • 5- Subcutaneous nodules : appear on the extensor surface of tendons near bony prominences.
Strep throat Antibody production Antibody cross-reaction with heart vegetations Aschoff body pericarditis
Minor criteria of rheumatic fever • Previous history of rheumatic fever • Arthralgia • Fever • Lab tests indicative of inflammation : increase ESR (erythrocyte sedimentation rate), CRP (C-Reactive protein), leukocytosis • Echocardiogram (ECG) changes
RHEUMATIC HEART DISEASE • It is a heart disease caused by rheumatic fever. • Rheumatic heart disease can be acute or chronic. • The incidence and mortality of rheumatic fever has declined over the past 30 years due to improved socioeconomic condition and rapid diagnosis and treatment of group A beta hemolytic streptococcus infection of the Pharynx or skin.
Effects of Rheumatic Fever on the Heart It affects all the 3 layers of the heart; • Affect the heart during its acute phase acute rheumatic carditis/ pancarditis(inflammation of endocardium, myocardium and pericardium) 1- Endocarditis — vegetations due to edema, and fibrin deposits on valve leaflets along lines of closure. Mostly mitral and aortic valve. • 2 - Myocarditis- Aschoff body which consists of a focus of necrosis (representing the site of antibody-antigen reaction) surrounded by activated histiocytes and lymphocytes. The histiocytes may be mononuclear or multinuclear, and are referred to as Anitschkow's or Aschoff cells. .
Small vegetations (verrucae) are visible along the line of closure of the mitral valve leaflet (arrowheads). Previous episodes of rheumatic valvulitis have caused fibrous thickening and fusion of the tendinous cords.
Microscopic appearance of an Aschoff body in a patient with acute rheumatic carditis. The myocardial interstitium has a circumscribed collection of mononuclear inflammatory cells, including some large histiocytes with prominent nucleoli, a prominent binuclear histiocyte, and central necrosis.
Acute rheumatic carditis 3- Pericarditis — "bread and butter appearance", due to fibrinous inflammation and deposition of fibrin on surface of pericardium. • Acute changes may resolve completely or progress to scarring and development of chronic valvular deformities many years after the acute disease
CHRONIC RHEUMATIC HEART DISEASE Manifests years or decades after the initial episode of rheumatic fever. The distribution of valve involvement is variable: • mitral alone: most common • combined mitral/aortic • pulmonary: very rare
Affection of the Aortic Valve in rheumatic carditis • Associated with mitral valve damage is usually present. • Aortic stenosis: • Aortic regurgitation
Complications of CHRONIC RHEUMATIC HEART DISEASE • Valvular Endocarditis heals by progressive fibrosis leading to Irreversible deformity in the form of: a- stenosis (Reduction of diameter): fish mouth (button hole) stenosis b- regurgitation (improper closure) : if fibrosis occurred in chordae tendonae so leaflets are retracted. • affection of the cardiac valves can also lead to cardiac failure secondary to ventricular hypertrophy then dilatation, thromboembolism and infective endocarditis,pulmonary congestion and hypertension.
surgically removed specimen of rheumatic aortic stenosis demonstrating thickening and distortion of the cusps with commissural fusion .
Chronic Rheumatic Carditis: • Signs and symptoms depend on the valve(s) involved: cardiac murmurs, ventricular hypertrophy then dilatation ending into heart failure, • arrhythmia, thromboembolism and infective endocarditis. • Treatment may require valve surgery.
Rheumatic Fever: summary • Body makes antibody to strep. bacteria that cross-reacts with antigens in heart and joints • 2-3 weeks after strep throat, patient gets: • migratory polyarthritis • pericardial friction rub, arrhythmias • Chronic disease can reappear decades later • mitral stenosis, left atrial enlargement, thrombi • increased risk of infective endocarditis
Diffferential diagnosis for rheumatic Endocarditis • Inflammation of the endocardium can also be caused by: • (A)Non-infective causes: • 1-Non-infective thrombotic endocarditis • 2- Libmann sacks verrucous endocarditis • (B)Infective causes: • 1 -Acute Infective endocarditis • 2 -Sub-acute Infective endocarditis
1-Nonbacterial Thrombotic EndocarditisNBTE • causes: • endothelial abnormalities ,Hypercoagulability. • Association with malignancy (50%). • Characterized by the deposition of small masses of fibrin, platelets, and other blood components on the leaflets of the cardiac valves (sterile thrombus). There is no infective organism. It is aseptic. • Aortic valve most common site. • Clinically asymptomatic, if large: may embolise, may become infected
2- (Libman-Sacks) verrucousendocarditis Less common, occur in patients with systemic lupus erythematosus due to deposition of circulating immune complexes in the valves.
B- Infective Endocarditis • Definition: infection of the cardiac valves or mural surface of the endocardium, resulting in the formation of vegetations (adherent mass of thrombotic debris and organisms). • Divided into: • Acute infective endocarditis: caused by highly virulent organisms (staphylococcus aureus)as apart of septicemia, infect even normal valves, progress rapidly. • Subacute infective endocarditis : infection of previously abnormal valves by organisms of low virulence (-hemolytic streptococci) as apart of bacteremia complicating i.v. drug abusers, previous dental, surgical procedure (catheterization)., progress slowly.
people at Risk for Subacute Infective Endocarditis: • Persons with cardiac abnormalities: e.g.chronic valvular diseases, septal defects etc. • Prosthetic heart valves. • Intravenous drug abusers.
Infective Endocarditis: Morphology • Aortic and mitral valves are the most common sites affected while right side valves commonly affected in i.v.users. • Vegetations may be single or multiple, involve one or more valve(s), differ in appearance according to the causative agent.
Infective Endocarditis: Morphology • In acute IE vegetations may: a- obstruct valve orifice b- lead to rupture of the leaflets, cordaetendineae, or papillary muscles c- abscess in perivalvular tissue (ring abscess) friable large yellow vegetations may become systemic emboli infarcts + abscesses. • In subacute IE vegetations are firmer, less destructive, and ring abscess are uncommon.
Endocarditis of the mitral valve (subacute, caused by Streptococcus viridens).
Histologic appearance of vegetation of endocarditis with extensive acute inflammatory cells and fibrin. Bacterial organisms were demonstrated by tissue Gram stain.
Gross photograph illustrating healed endocarditis with perforations on bicuspid aortic valve.
comparison of the lesions in the four major forms of vegetative endocarditis 1- rheumatic heart disease: vegetations are marked by a row of warty, small vegetations along the lines of closure of the valve leaflets. 2- IE (infective endocarditis): vegetations are characterized by large, irregular masses on the valve cusps that can extend onto the cords .
3- NBTE (nonbacterial thrombotic endocarditis) typically exhibits medium sized bland vegetations, usually attached at the line of closure. 4-LSE (Libman-Sacks endocarditis) has small or medium-sized vegetations on either or both sides of the valve leaflets.