Download
1 / 1
10 likes | 168 Views
Observational Study to determine if Chorionicity, in Planned Vaginal delivery affects labour and neonatal outcome Quek Y.S. (1), Woon S.Y. (1), Ravichandan N. (2), Kaliammah MK (1), Shantala V. (3), Ravichandran J. (1)

E N D
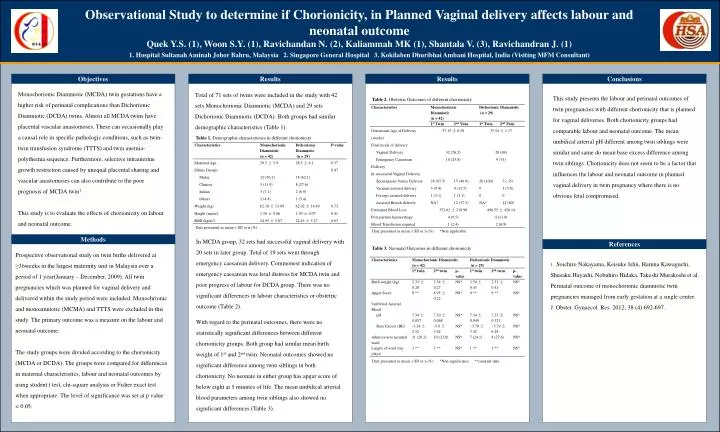
Observational Study to determine if Chorionicity, in Planned Vaginal delivery affects labour and neonatal outcome Quek Y.S. (1), Woon S.Y. (1), Ravichandan N. (2), Kaliammah MK (1), Shantala V. (3), Ravichandran J. (1) 1. Hospital Sultanah Aminah Johor Bahru, Malaysia 2. Singapore General Hospital 3. Kokilaben Dhuribhai Ambani Hospital, India (Visiting MFM Consultant) OPTIONALLOGO HERE OPTIONALLOGO HERE Objectives Results Results Conclusions Monochorionic Diamniotic (MCDA) twin gestations have a higher risk of perinatal complications than Dichorionic Diamniotic (DCDA) twins. Almost all MCDA twins have placental vascular anastomoses. These can occasionally play a causal role in specific pathologic conditions, such as twin-twin transfusion syndrome (TTTS) and twin anemia-polythemia sequence. Furthermore, selective intrauterine growth restriction caused by unequal placental sharing and vascular anastomoses can also contribute to the poor prognosis of MCDA twin1. This study is to evaluate the effects of chorionicity on labour and neonatal outcome. Total of 71 sets of twins were included in the study with 42 sets Monochorionic Diamniotic (MCDA) and 29 sets Dichorionic Diamniotic (DCDA). Both groups had similar demographic characteristics (Table 1). This study presents the labour and perinatal outcomes of twin pregnancies with different chorionicity that is planned for vaginal deliveries. Both chorionicity groups had comparable labour and neonatal outcome. The mean umbilical arterial pH different among twin siblings were similar and same do mean base excess difference among twin siblings. Chorionicity does not seem to be a factor that influences the labour and neonatal outcome in planned vaginal delivery in twin pregnancy where there is no obvious fetal compromised. Table 2. Obstetric Outcomes of different chorionicity Table 1. Demographic characteristics in different chorionicity Data presented as mean ± SD or n (%). Data presented as mean ± SD or n (%). *Non-applicable Methods In MCDA group, 32 sets had successful vaginal delivery with 20 sets in later group. Total of 19 sets went through emergency caesarean delivery. Commonest indication of emergency caesarean was fetal distress for MCDA twin and poor progress of labour for DCDA group. There was no significant differences in labour characteristics or obstetric outcome (Table 2). With regard to the perinatal outcomes, there were no statistically significant differences between different chorionicity groups. Both group had similar mean birth weight of 1st and 2nd twin. Neonatal outcomes showed no significant difference among twin siblings in both chorionicity. No neonate in either group has apgar score of below eight at 5 minutes of life. The mean umbilical arterial blood parameters among twin siblings also showed no significant differences (Table 3). References Table 3. Neonatal Outcomes in different chorionicity Prospective observational study on twin births delivered at ≥36weeks in the largest maternity unit in Malaysia over a period of 1 year(January – December, 2009). All twin pregnancies which was planned for vaginal delivery and delivered within the study period were included. Monochrionic and monoamniotic (MCMA) and TTTS were excluded in this study. The primary outcome was a measure on the labour and neonatal outcome. The study groups were divided according to the chorionicity (MCDA or DCDA). The groups were compared for differences in maternal characteristics, labour and neonatal outcomes by using student t test, chi-square analysis or Fisher exact test when appropriate. The level of significance was set at p value < 0.05. 1. Soichiro Nakayama, Keisuke Ishii, Haruna Kawaguchi, Shusaku Hayashi, Nobuhiro Hidaka, Takeshi Murakoshi et al. Perinatal outcome of monochorionic diamniotic twin pregnancies managed from early gestation at a single center. J. Obstet. Gynaecol. Res 2012; 38 (4):692-697. Data presented as mean ± SD or n (%). *Non-significance **constant data






















