Download
1 / 40
400 likes | 481 Views
Health Care Access after Spinal Cord Injury. Lee L. Saunders, PhD Medical University of South Carolina. Acknowledgement.

E N D
Health Care Access after Spinal Cord Injury Lee L. Saunders, PhD Medical University of South Carolina
Acknowledgement • The contents of this presentation were developed under grants from the Department of Education, NIDRR grant numbers H133G050165, H133B090005, and H133A080064, and the National Institutes of Health, grant number 1R01 NS 48117. However, those contents do not necessarily represent the policy of the Department of Education or NIH, and you should not assume endorsement by the Federal Government.
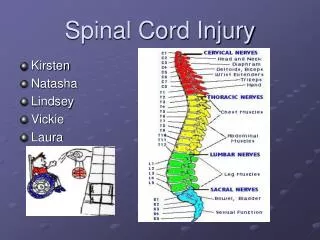
Spinal Cord Injury (SCI) • Results in immediate and general permanent changes in sensory, motor, bowel, bladder, and sexual function • Risk of secondary conditions and early mortality • 12,000 new cases per year • 265,000 living with spinal cord injury (SCI) in the US • Average age at injury = 40.7 years • 80.7% male • 66.5% White, 26.8% African-American National Spinal Cord Injury Statistical Center, Facts and Figures 2011
Health Care Access (HCA) • The ability of a person to receive health care services • Availability of personnel and supplies • Ability to pay for services
Health Care Access and SCI • People with disabilities have reported three times more unmet health needs than the general population (Beatty et al., 2003; Donnelly et al., 2007). • One survey study (Shigaki et al., 2002) suggested those with SCI had difficulty in accessing services (87% of survey population). • Beatty et al. (2003), only half of the individuals who requested a need for rehabilitation services received them every time they were requested, regardless of health plan type. • Medicare remains the largest payer of specific rehabilitation services, and Medicare payment policies continue to have an impact on willingness of providers to supply rehabilitation services (Dejong et al., 2002).
Health Care Access and Insurance Type • Research on health care access (HCA) and outcomes after SCI has mainly focused on insurance type. • Insurance type has been linked with re-hospitalization after rehabilitation, length of stay during rehabilitation (DeVivo 1989), psychological distress, and participation (Tate 1994). • Lack of insurance, in addition to racial-ethnic minority status and low income, is associated with barriers to HCA (Neri 2003).
HCA and Secondary Conditions • Access to care is a critical, yet understudied, factor in relation to secondary conditions after SCI (Beatty et al., 2003; Donnelly et al., 2007; Neri & Kroll, 2003b; Shigaki, Hagglund, Clark, & Conforti, 2002). • Low income (proxy variable for poor access to services) has been linked to early mortality after SCI (Krause, Zhai, Saunders, & Carter, 2009), and secondary conditions are the primary predictors of mortality (Krause, Carter, Pickelsimer, & Wilson, 2008; Krause et al., 2009).
Association of Race, Socioeconomic Status, and Health Care Access with Pressure Ulcers after SCI Saunders LL, Krause KS, Acuna J. (2012). Association of race, socioeconomic status, and health care access with pressure ulcers after spinal cord injury. Archives of Physical Medicine and Rehabilitation, 93:972-7.
Background • Pressure ulcers (PrU) are one of the most common secondary conditions after SCI • Associated with significant costs (Javits, 1998) and are linked with early mortality (Krause, 2009)
Background • Lack of money, insurance, and transportation linked with not being able to see a physician to heal a PrU (Saladin, 2009) • Primary care at baseline associated with lower odds of PrU at follow-up 1 year later (Kroll, 2007)
Background • Race has been found to be significantly associated with pressure ulcer (PrU) outcomes after SCI (Saunders, 2010). • Socioeconomic status (SES), as measured by income and education, was also found to be associated with PrU outcomes, and mediated the relationship between race and PrU outcomes. • Study did not take HCA into account.
Study Objective • To assess the association of race, SES, and HCA with PrU outcomes
Procedures • IRB approval obtained • Introductory letters were sent to potential participants, followed by the survey 2 weeks later. • $50 remuneration
Participants • Participants were identified from a large specialty hospital in the southeastern USA. • All participants had traumatic SCI, were a minimum of 1 year post-injury, and were 18 years or older at assessment. • Out of 3669 potential participants, 2549 eligible persons responded to a mail-in survey (69.5% response rate).
PrU Outcomes • Current PrU (yes, no) • Number of days sitting time affected by PrU in the past year (no PrU in the past year, no reduced sitting time, a month or less, more than a month) • Surgery to repair a PrU since SCI onset (yes, no)
Variables • Demographic/Injury: • Race (White, Black, other) • Gender (male, female) • Injury severity (C1-C4, non-ambulatory; C5-C8, non-ambulatory; Non-cervical, non-ambulatory; Ambulatory) • Age • Years since injury • SES • Education (<high school, high school, <bachelor’s, bachelors+) • Household income (<$25K, $25-$75K, $75K +) • HCA • Health care coverage (yes, no) • Personal health care doctor (yes, no) • Could not see doctor in past 12 months because of cost (yes, no)
Analysis • Two-stage logistic regression models for 2 outcomes (current PrU, PrU surgery) • Multinomial logistic regression for 1 outcome (reduced sitting time) • Stage 1: Base model with demographic and injury characteristics and SES • Stage 2: HCA items added to Stage 1
Results: Participant Characteristics • Male = 75.2% • White = 72.3% • Average age = 45.6 years • Ambulatory = 30.9% • Of the non-ambulatory: • 10.8% had C1-C4 injury • 25.1% had C5-C8 injury • 33.3% non-cervical injury • 15.3% reported having less than a high school degree; 27.3% had a bachelor’s degree • Household income of $75,000 or more was reported by 22% of participants, 39.2% reported less than $25,000
Results • Current PrU • 39.3% participants reported a PrU in the past year, 19.9% had a current PrU • Reduced Sitting time Due to PrU in Past year • 10.4% participants reported reduced sitting time by more than a month • 12.2% had sitting time reduced by a month or less • 16.6% had no reduced sitting time • 60.8% had no PrU in the past year • PrU Surgery since SCI Onset • 21.9% reported having had surgery for a PrU since their SCI onset
Results: Current PrU Odds ratios and 95% CIs for having a current PrU (yes vs. no)*
Results: Reduced Sitting Time Stage 1 Multinomial regression model results for having reduced sitting time due to a PrU in the past year*
Results: Reduced Sitting Time Stage 2 Multinomial regression model results for having reduced sitting time due to a PrU in the past year (yes vs. no)*
Results: PrU Surgery Logistic regression model results for having had surgery for a PrU since SCI onset (yes vs. no)*
Conclusions • Even after accounting for HCA, SES, specifically household income, remained significantly associated with PrU outcomes after SCI. • No relationship was found between race or education and PrU outcomes after controlling for income. • Health care providers should be aware of the increased risk of PrU in lower SES populations, even after accounting for HCA.
Limitations • Self-report data • Unable to assess the severity or grade of reported PrUs • Cross-sectional data • Participants identified through a clinical setting • Limited scope of HCA measures
Healthcare Access after Spinal Cord Injury: A Comparison with the General Population
Background • Substantial racial-ethnic differences have been noted in the availability and delivery of healthcare. • African-Americans are less likely to have a regular medical doctor, to be able to pay for needed medication, and report lower satisfaction for all areas of healthcare (Lasser et al., 2006). • Convenience and availability (transportation, needed medical services, hours) appear to be more prominent barriers for African-Americans,(Larson et al., 2007) as are affordability and lack of health insurance (Wheeler et al., 2007).
Objective • To identify the extent to which African-Americans with SCI have equal HCA compared to African-Americans in the general population.
Procedures • IRB approval obtained • Mail-in survey to potential participants using questions from the Behavioral Risk Factor Surveillance System (BRFSS) • $50 remuneration
SCI Participants • South Carolina SCI Surveillance System Registry • Identified through hospital discharge and emergency department discharge records • 18 years or older, African-American • ICD-9-CM Codes – 806 [.0-.9]; 952 [.0-.9] • All persons discharged between 2002-2009 still alive at the time of survey were approached.
Behavioral Risk Factor Surveillance System • 2009 BRFSS data downloaded from the CDC website • 18 years or older • African-American • South Carolina resident
BRFSS Identified HCA Questions • Do you have any kind of health care coverage? • Yes, No • Do you have one person you think of as your personal doctor? • Yes (one), Yes (more than one), No • Was there a time in the past 12 months you could not see a doctor because of cost? • Yes, No • About how long has it been since you last visited a doctor for a routine checkup? • Never, Past year, Past 2 years, Past 5 years, 5+ years ago
Personal Doctor • Persons with SCI were: • Less likely to have one person they thought of as their personal doctor • More likely to have more than one person they thought of as their personal doctor
Health Care Coverage • Among those with SCI who reported no health care coverage: • Time since healthcare coverage • 12.5% had coverage in the past year • 37.5% reported 5 or more years since having coverage • Main reason without healthcare coverage • 34.5% - lost job or change in employer • 17.2% - cannot afford premiums • 10.3% - employer does not offer coverage
Health Care Coverage • Those who were able to walk were less likely (74.7% vs. 91.4%) to have healthcare coverage (p=0.0063). • Men were less likely to have coverage than women (78.3% s. 93.9%; p=0.0380). • Having health care coverage did not differ by employment or education.
Conclusions • Persons with SCI are a vulnerable population, and reduced access to health care could create even wider disparities in health outcomes. • We found differences with regards to time since last routine check-up as well as having a personal health care doctor.
Future Studies • Expanded measures of health care coverage, including physical barriers as well as access to rehabilitation therapy and proper equipment • Longitudinal data to asses changes in health care access and coverage
Longevity after Injury Project Interested in more information? • Lee Saunders: saundel@musc.edu • Website: http://www.musc.edu/chp/sciorg