Download
1 / 40
600 likes | 1.7k Views
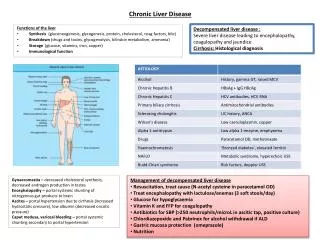
Treatment of chronic liver disease. Treatment. Cause ( Etiology) Complication. Etiology. Infection Alcohol Autoimmune Cholestatic Infiltrative Metabolic Vascular Drugs. Complications. Ascites GI bleed SBP Edema Hepatoma Encephalopathy Hepatorenal syndrome. Hepatitis B

E N D
Treatment • Cause ( Etiology) • Complication
Etiology • Infection • Alcohol • Autoimmune • Cholestatic • Infiltrative • Metabolic • Vascular • Drugs
Complications • Ascites • GI bleed • SBP • Edema • Hepatoma • Encephalopathy • Hepatorenal syndrome
Hepatitis B Nucleoside analogues Lamivudine Adefovir Telbivudine Entecavir Tenofovir Interferon Hepatitis C Alfa interferon Pegylated interferon Ribavirin Viral hepatitis
Autoimmune hepatitis Prednisone Azathioprine New drugs Budesonide Cyclosporine Tacrolimus Rapamycin Mycophenolate mofetil NAFLD Weight loss Underlying disease Silymarin/metformin Bariatric surgery
Alcohol Abstinence Fatty liver Liver transplant Wilson disease Penicillamine Trientine Zinc acetate Tetrathiomolybdate Family screening
PBC Ursodeoxycholic acid Symptomatic Cholestyramine/Rifampicin Calcium/vitamin D PSC ERCP Liver transplant Hemochromatosis Phlebotomy Family screening Alpa1 antitrypsin deficiency 4-phenylbutyric acid Liver transplant Genetic counseling
COMPLICATIONS OF CIRRHOSIS Complications of Cirrhosis Result from Portal Hypertension or Liver Insufficiency Variceal hemorrhage Portal hypertension Spontaneous bacterial peritonitis Ascites Cirrhosis Hepatorenal syndrome Encephalopathy Liver insufficiency Jaundice
MECHANISM OF ACTION OF ENDOSCOPIC THERAPY IN PORTAL HYPERTENSION Splanchnic arteriolar resistance Resistance to portal flow Resistance to portal flow Variceal Band Ligation or Sclerotherapy Portal blood inflow Portal pressure Varices/ Variceal Hemorrhage Variceal obliteration Cirrhosis
PROGNOSTIC INDICATORS OF FIRST VARICEAL HEMORRHAGE Varix with red signs Variceal hemorrhage • Predictors of hemorrhage: • Variceal size • Red signs • Child B/C NIEC. N Engl J Med 1988; 319:983
MANAGEMENT OF PATIENTS WITH VARICES WHO HAVE NEVER BLED Management depends on the size of varices Treatment of Varices / Variceal Hemorrhage No varices Varices No hemorrhage Variceal hemorrhage Recurrent hemorrhage
MANAGEMENT OF PATIENTS WITH MEDIUM/LARGE VARICES WITHOUT PRIOR HEMORRHAGE 1) -blockers (propranolol, nadolol) indefinitely 2) Endoscopic Variceal Ligation in patients intolerant to -blockers Treatment of Varices / Variceal Hemorrhage No varices Small varices No hemorrhage Medium/ large varices No hemorrhage Variceal hemorrhage Recurrent hemorrhage
CONTROL OF ACUTE VARICEAL HEMORRHAGE Control of hemorrhage Treatment of Varices / Variceal Hemorrhage No varices Small varices No hemorrhage Medium/ large varices No hemorrhage Variceal hemorrhage Recurrent hemorrhage
TREATMENT OF ACUTE VARICEAL HEMORRHAGE Treatment of Acute Variceal Hemorrhage General Management: • IV access and fluid resuscitation • Do not over transfuse (hemoglobin ~ 8 g/dL) • Antibiotic prophylaxis Specific therapy: • Pharmacological therapy: Terlipressin, Somatostatin and analogues, Vasopressin + Nitroglycerin • Endoscopic therapy: Ligation, Sclerotherapy • Shunt therapy: TIPS, surgical shunt
ENDOSCOPIC VARICEAL BAND LIGATION Endoscopic Variceal Band Ligation • Bleeding controlled in 90% • Rebleeding rate 30% • Compared with Sclerotherapy: • Less rebleeding • Lower mortality • Fewer complications • Fewer treatment sessions
THE TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT Transjugular Intrahepatic Porto systemic Shunt Hepatic vein TIPS Splenic vein Portal vein Superior mesenteric vein
ENDOSCOPIC IMAGES OF GASTRIC VARICES Gastric Varices Pretreatment cyanoacrylate Post-treatment cyanoacrylate
Mild and SeverePortal Hypertensive Gastropathy ENDOSCOPIC IMAGES OF MILD AND SEVERE PORTAL HYPERTENSIVE GASTROPATHY Mild Severe Mosaic pattern Mosaic pattern + red spots Carpinelli et al. Ital J Gastroenterol Hepatol 1997; 29:533
ASCITES AND HEPATORENAL SYNDROME Ascites and Hepatorenal Syndrome
NATURAL HISTORY OF ASCITES Natural History of Ascites Portal Hypertension No Ascites HVPG <10 mmHg Mild Vasodilation Uncomplicated Ascites HVPG >10 mmHg Moderate Vasodilation Refractory Ascites HVPG >10 mmHg Severe Vasodilation HVPG >10 mmHg Extreme Vasodilation Hepatorenal Syndrome
DIAGNOSTIC PARACENTESIS Diagnostic Paracentesis Indications • New-onset ascites • Admission to hospital • Symptoms/signs of SBP • Renal dysfunction • Unexplained encephalopathy Contraindications • None
MANAGEMENT OF UNCOMPLICATED ASCITES Management of Uncomplicated Ascites Definition: Ascites responsive to diuretics in the absence of infection and renal dysfunction Sodium restriction • Effective in 10-20% of cases • Predictors of response: mild or moderate ascites, Urine Na excretion > 50 mEq/day Diuretics • Should be spironolactone-based • A progressive schedule (spironolactone furosemide) requires fewer dose adjustments than a combined therapy (spironolactone + furosemide)
MANAGEMENT OF UNCOMPLICATED ASCITES: SODIUM RESTRICTION Management of Uncomplicated Ascites Sodium Restriction • 2 g (or 5.2 g of dietary salt) a day • Fluid restriction is not necessary unless there is hyponatremia (<125 mmol/L) • Goal: negative sodium balance
MANAGEMENT OF UNCOMPLICATED ASCITES: DIURETIC THERAPY Management of Uncomplicated Ascites Diuretic Therapy Dosage • Spironolactone 100-400 mg/day • Furosemide (40-160 mg/d) for inadequate weight loss or if hyperkalemia develops • Increase diuretics if weight loss <1 kg in the first week and < 2 kg/week thereafter • Decrease diuretics if weight loss >0.5 kg/day in patients without edema and >1 kg/day in those with edema • Side effects • Renal dysfunction, hyponatremia, hyperkalemia, encephalopathy, gynecomastia
DEFINITION AND TYPES OF REFRACTORY ASCITES 80% 20% Definition and Types of Refractory Ascites Occurs in ~10% of cirrhotic patients • Diuretic-intractable ascites Therapeutic doses of diuretics cannot be achieved because of diuretic-induced complications • Diuretic-resistant ascites No response to maximal diuretic therapy (400 mg spironolactone + 160 mg furosemide/day)
SPONTANEOUS BACTERIAL PERITONITIS (SBP) COMPLICATES ASCITES AND CAN LEAD TO RENAL DYSFUNCTION Portal Hypertension No Ascites HVPG <10 mmHg Mild Vasodilation Uncomplicated Ascites HVPG >10 mmHg Moderate Vasodilation Refractory Ascites SBP HVPG >10 mmHg Severe Vasodilation HVPG >10 mmHg Extreme Vasodilation Hepatorenal Syndrome Spontaneous Bacterial Peritonitis (SBP) Complicates Ascites and Can Lead to Renal Dysfunction
EARLY DIAGNOSIS OF SPONTANEOUS BACTERIAL PERITONITIS (SBP) Early Diagnosis of SBP • Diagnostic paracentesis: • If symptoms / signs of SBP occur • Unexplained encephalopathy and / or renal dysfunction • At any hospital admission • Diagnosis based on ascitic fluid PMN count >250/mm3
MICROORGANISMS ISOLATED IN SPONTANEOUS BACTERIAL PERITONITIS (SBP) Microorganisms Isolated in Spontaneous Bacterial Peritonitis Microorganism % of Cases Gram-negative bacilli 72 Gram-positive cocci 29
TREATMENT OF SPONTANEOUS BACTERIAL PERITONITIS (SBP) Treatment ofSpontaneous Bacterial Peritonitis • Recommended antibiotics for initial empiric therapy • i.v. cefotaxime, • i.v. amoxicillin-clavulanic acid • avoid aminoglycosides • Minimum duration: 5 days
INDICATIONS FOR PROPHYLACTIC ANTIBIOTICS TO PREVENT SPONTANEOUS BACTERIAL PERITONITIS (SBP) Indications for Prophylactic Antibiotics to Prevent Spontaneous Bacterial Peritonitis • Patients who have recovered from SBP (long-term) • Norfloxacin 400 mg p.o. daily, indefinitely • Weekly Quinolones
CHARACTERISTICS OF HEPATORENAL SYNDROME (HRS) Characteristics of Hepatorenal Syndrome • Renal failure in patients with cirrhosis, advanced liver failure and severe sinusoidal portal hypertension • Absence of significant histological changes in the kidney (“functional” renal failure) • Marked arteriolar vasodilation in the extra-renal circulation • Marked renal vasoconstriction leading to reduced glomerular filtration rate
TYPES OF HEPATORENAL SYNDROME (HRS) Two Types of Hepatorenal Syndrome Type 1 • Rapidly progressive renal failure (2 weeks) • Doubling of creatinine to >2.5 Type 2 • More slowly progressive • Creatinine >1.5 mg/dL or Creatinine Clearance < 40 ml/min • Associated with refractory ascites
MANAGEMENT OF HEPATORENAL SYNDROME Management of Hepatorenal Syndrome Proven efficacy • Liver transplantation Under investigation • Vasoconstrictor + albumin • Transjugular intrahepatic portosystemic shunt (TIPS) • Vasoconstrictor + TIPS • Extracorporeal albumin dialysis (ECAD) Ineffective • Renal vasodilators (prostaglandin, dopamine) • Hemodialysis
PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY Pathophysiology of Hepatic Encephalopathy Ammonia Upregulation of astrocytic peripheral benzodiazepine receptors (PBR) Neurosteroid production Modulation of GABA receptor Hepatic encephalopathy
HEPATIC ENCEPHALOPATHY IS A CLINICAL DIAGNOSIS Hepatic Encephalopathy is a Clinical Diagnosis • Clinical findings and history important • Ammonia levels are unreliable • Ammonia has poor correlation with diagnosis • Measurement of ammonia not necessary • Number connection test • Slow dominant rhythm on EEG
STAGES OF HEPATIC ENCEPHALOPATHY Stages of Hepatic Encephalopathy Confusion Drowsiness Somnolence Coma 1 2 3 4 Stage
TREATMENT OF HEPATIC ENCEPHALOPATHY Treatment of Hepatic Encephalopathy • Identify and treat precipitating factor • Infection • GI hemorrhage • Prerenal azotemia • Sedatives • Constipation • Lactulose (adjust to 2-3 bowel movements/day) • Protein restriction, short-term (if at all)
Liver transplant • All patients with end stage liver disease should be assessed for liver transplant when ever is proven to significantly prolong survival and improve quality of life in a coast effective manner over natural history of the liver disease and other medical and non transplant surgical intervention.