Download
1 / 12
140 likes | 325 Views
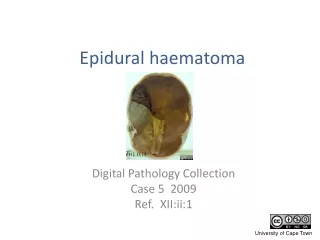
Epidural Abcess. Note: Dura adheres to the skull above the foramen magnum and anteriorly down to L1. Mechanism of Damage. Direct compression Thrombosis and thrombophlebitis of nearby veins Interruption of the arterial blood supply Focal vasculitis

E N D
Note: Dura adheres to the skull above the foramen magnum and anteriorly down to L1
Mechanism of Damage • Direct compression • Thrombosis and thrombophlebitis of nearby veins • Interruption of the arterial blood supply • Focal vasculitis • Bacterial toxins and mediators of inflammation
Epidemiology • Incidence- 25/100,000 hospital admissions • 0.5-3% of patients with long term epidural catheters
Microbiology • Staphylococcus aureus — 63 percent • Gram negative bacilli — 16 percent • Streptococci — 9 percent • Coagulase-negative staphylococci — 3 percent, mostly occurring in patients with prior spinal instrumentation • Anaerobes — 2 percent • Others — 1 percent • Unknown — 6 percent • Mycobacteria- excluded in this list, but important in developing nations
Sources of Infection • No source ID’d- 30 % • Skin and soft tissue infxn- 22 % • Spinal surgery- 12 % • IVDU 10 % • Other, including epidural catheters- 8 % • Bone or Joint- 7 % • UTI, URI, Sepsis, Abdomen, and other catheters each make up adt’l < 3%
Clinical Presentation • Classic Triad: • Fever • Back Pain • Neurologic Deficit • Progression: Back pain root pain motor/sensory/bowel bladder paralysis
Delays in Diagnosis • 63 SEA patients matched to 126 controls with spine pain • Diagnostic delays in 75% of SEA patients. • Residual motor weakness in 45% vs. only 13% of patients without diagnostic delays (p < 0.05). • “Classic triad" in 13% of SEA patients and 1% of controls during the initial visit (p < 0.01) • > 1 RF’s in 98% of SEA patients and 21% of controls (p < 0.01) • RF’s-DM,IVDU, liver disease, renal failure, indwelling catheter, immunocompromised, recent invasive spinal procedure, vertebral fracture, and distant site of infection The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. Davis DP; Wold RM; Patel RJ; Tran AJ; Tokhi RN; Chan TC; Vilke GM. J Emerg Med 2004 Apr;26(3):285-91.
Therapy • Principles: • Reduction of the inflammatory mass • Eradication of the causative organism • Empiric Abx: • Nafcillin plus metronidazole plus either cefotaxime or ceftazidime • Vancomycin (1 g every 12 hours) can be substituted for nafcillin • Tx X 4-6 W or until improvement on MRI
Therapy • A retrospective analysis of 57 cases tx’d over 14 y in S.Dakota • The lumbar region was most frequently involved, and 46% of patients were immunocompromised. Staphylococcus aureus was the most frequently encountered pathogen. • For 60 treatment courses, management included medical only (25 patients), medical plus computed tomography-guided percutaneous needle aspiration (7 patients), or surgical drainage approaches (28 patients). • Prolonged use of antibiotics alone or combined with percutaneous needle drainage yielded clinical outcomes comparable with antibiotics plus surgical intervention, irrespective of patient age, presence of comorbid illness, disease onset, neurologic abnormality at time of presentation, or abscess size. • Medical vs surgical management of spinal epidural abscess. Siddiq F; Chowfin A; Tight R; Sahmoun AE; Smeg RA Jr Arch Intern Med 2004 Dec 13-27;164(22):2409-12.
References • www.uptodate.com, unless otherwise noted