Download
1 / 58
670 likes | 816 Views
Discover the unique anatomical & physiological features of respiratory systems in children vs. adults. Learn the clinical implications, chest wall mechanics, and challenges in providing physiotherapy care for children. Understand the impact of preferential nasal breathing on pediatric respiration.

E N D
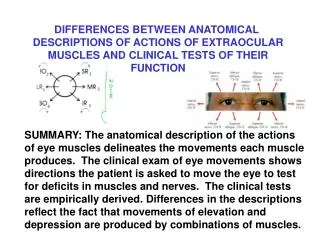
Respiratory System:Anatomical and Physiological differences between adults and children Robyn Smith Department of Physiotherapy UFS 2012
Learning outcomes • At the end of this module the learner should: • Be able to identify both key anatomical and physiological differences between the respiratory systems of child and a adult • Understand and explain the impact of these differences on the clinical findings, observations and respiration of a child • Describe the impact of preferential nasal breathing on respiration in babies
The main reason for hospital admissions in children under the age of 4 years worldwide is respiratory illness
Background • The respiratory system of children differs both anatomically and physiologically from that of adults • These differences have important consequences for the physiotherapy care of children in terms of assessment, treatment and choice of techniques
Background • The principles of adult chest physiotherapy cannot be directly transposed to a child. • Chest physiotherapy as provided to children has become a specialised area on its own for this reason
Mechanics of respiration • Air moves in and out of the lungs due to changes in pressure gradients created by movement of the chest wall and muscular action • Inspiration active process • Diaphragm • Intercostals • Accessory muscles • Expiration is passive • Forced expiration involves abdominal muscles e.g. cough
Components of respiratory system • Most of the components of the respiratory system are present at birth but • are underdeveloped, • and immature • This poses certain challenges to the child regarding breathing
Anatomical differences include: • The chest or thorax • Shape • Ribcage • Mechanism of breathing • Breathing pattern • Diaphragm • Internal organs • Airway diameter • Bronchial walls • Surfactant • Alveoli • Collateral ventilation • Exposure to toxins and allergens
Thorax: Chest shape • Cross sectional area of the thorax is cylindrical and not elliptical as in adults
Infant chest shape • Anterior view • Lateral view
Thorax: Ribcage • The ribcage of the newborn and infant is relatively soft and cartilaginouscompared to the rigid chest wall of older children and adults • Ribs run horizontally to the vertebrae and sternum compared to the more oblique angle of older children and adults.
Thorax: Ribcage • The bucket handle movement of ribcage as seen in older children and adults is therefore not possible. • This mechanism is used to increase lung volumes during inspiration.
Thorax: Ribcage • Infant can therefore only increase the anterior-posterior or transverse diameter of their chest • The intercostal muscles are inactive and poorly developed in infancy. • The abdominal muscles are not yet stabilising the ribcage (only from about 3-4 months) • The interaction of gravity and the musculoskeletal system play an important role in the development of the thorax.
Thorax.... clinical implications • With the limited chest expansion the child can only increase their lung volumes by increasing their respiration rate, this explains why small children have a higher RR than adults • NB!!!! No head down position for postural drainage premature infants or neonates (1month). Even older infants need to monitored on how they copes when put in a head down position. • Infants are diaphragmatic breathers, therefore they are positioned in a head up position to ease the work of breathing
Thorax.... clinical implications • Premature infants & children with hypotonic need to be positioned correctly to avoid chest deformitiese.g. scoliosis or kyphosis • Rib flaring and a high riding ribcages are common in children with weak abdominal muscles and children with cerebral palsy as it does not anchor and pull down the ribcage • Infants with chronic cardio-respiratory conditions associated with prematurity or CHDparadoxal breathing may occur over a long period of time resulting in chest deformities forming over time e.g. pectusexcavatum or carniatum because the chest wall is still so pliable.
Flaring ribs Barrel chest Abnormal chest forms
Pectus carniatum Pectus excavatum Abnormal chest forms
Scoliosis Kyphosis Postural deformities
Preferential nasal breathing • Shape and orientation of the head and neck in babies means that the airway prone to obstruction • NB!!! Infants up to about 6 months are preferential nose breathers
Preferential nasal breathing ...clinical implications • Children with upper respiratory tract infections and nasal secretions may have compromised respiration if the nose is blocked • Constant oxygen therapy dries out the mucociliary escalator. • As physiotherapists we need to ensure adequate humidification e.g. saline inhalations or saline nose drops and • Keep the nose clear by suctioning or aspiration
Diaphragm • Angle of insertion of the diaphragm in infants is more horizontal • Diaphragm works at a mechanical disadvantage • Diaphragm in infants has a lower-content of high-endurance muscle fibresand also more susceptible to fatigue
Diaphragm • The diaphragm is the most important inspiratory muscle in children due to the immaturity and inactivity of the intercostal muscles • Weak accessory muscles and the abdominals as well in small babies
Diaphragm...clinical implications Ventilation is compromised in infants where the function of the diaphragm is impaired: Examples of such cases include: • abdominal distension • Phrenic nerve paralysis • When placed in the head down position • Congenital diaphragmatic hernia
Internal organs • Heart and other organs are relatively large in relation to the infants size
Internal organs... clinical implications This leaves less place for chest expansion
Airway diameter • Trachea is short and narrow about a 1/3 of diameter adult in neonate. • Generally all airways are narrower. • This makes respiratory resistance higher and the work of breathing greater. • Narrowest part of the airway is the cricoid ring • Right bronchus less angled • During the first few years of life there is significant growth in the diameter of the airways
Airway diameter...clinical implications • Tracheal swelling as a result of intubation can heighten the resistance • Inflexible cricoid ring leaves child more vulnerable to post extubation mucosal oedema and stridor • Children are often intubated into the right bronchus resulting in collapse of left lung • Children more likely to have tracheal injury after intubation (stenosis/ulceration)
Bronchial walls • Bronchial walls are supported by cartilaginous rings. However the support provided in children is far less than in adults making airways more prone to collapse • The bronchial wall has proportionally more cartilage, connective tissue and goblet cells than in adults and less muscle tissue is present • Beta adrenergic receptors are immature
Bronchial walls...clinical implications • Airways are more prone to collapse • Lung tissue less complaint • Less smooth muscles makes them less responsive to bronchodilator therapy until the age of 12 years (but especially in the first 1-2 years of life)
Cilia • At birth cilia are poorly developed
Cilia Clinical implication... • Ineffective mucociliary escalator • Risk of secretion retention and airway obstruction is greater in premature infants and neonates
Primary Ciliary Dyskinesia • Rare genetic disorder • Also known as Kartagener’s Syndrome • Cilial motility is severely reduced • Due to structural defect in the cilia • Results in recurrent sinusitis or bronchiectasis due to the impaired sputum clearance
Surfactant • Surfactant is a phospholipid produced by the type II pneumocytes in the lungs • Function is to reduce the surface tension at the air liquid interface in the alveoli making it easier to expand the alveoli • Secreted from 23 weeks gestation, with a surge in production at 30-34 weeks as the lungs become fully mature
Surfactant.... clinical implications • Premature infants have insufficient surfactant resulting in: • ↑ surface tension with alveoli that are difficult to expand • ↑ Work of breathing • more easily develop respiratory distress and-failure than adults • More easily develop atelectasis/lung collapse
Alveoli • Very few, small alveoli are present at birth • Alveoli develop after birth in terms of increasing numbers and in size. • The majority of the development occurs within the first 2 years. • Alveoli are important for gaseous exchange
Alveoli....clinical implications • Smaller alveoli in infants make them more susceptible to collapse and atelectasis • Smaller alveoli also provides a smaller area for gaseous exchange
Collateral ventilation • Ensures that distal lung units are ventilated despite the obstruction of a main airway • The collateral ventilatory channels are poorly developed in children under 2-3 years
Collateral ventilation.... clinical implications... • Makes the child more susceptible to alveolar collapse
Height and exposure to pollution • Children have a higher RR, spend more time outdoors exposing them to allergens and pollutants • Their height also exposes the child to other pollutants e.g. exhaust fumes • Passive smoking
Physiological differences include: • Lung compliance • V/Q matching • Closing volume • Oxygen consumption • Muscle endurance • Breathing pattern
Lung compliance • Measure of the pressure required to increase the volume air in the lungs • Combination of lung- and chest wall compliance • Lung compliance in a child is comparable to an adult and is directly proportional to the child’s size • Compliance in a child is reduced by the high proportion of cartilage in the airways • Premature infants with insufficient surfactant show reduced compliance
Chest wall compliance • The chest wall of the infant is cartilaginous and very soft and compliant. • In the case of respiratory distress the chest is drawn inwards. Substernal, subcostal and intercostal recession is common in such cases. • This is the reason for paradoxal breathing, if this persists over long period of time it can result in chest deformities