Download
1 / 43
430 likes | 687 Views
Board Responsibility for Medical Staff Privileges and Credentialing. Web Conference April 3, 2008 12 – 1 p.m. . For audio, call: 1-888-850-5066 code 222177#. Association of Washington Public Hospital Districts. Sponsored by:. Significant funding provided by:

E N D
Board Responsibility for Medical Staff Privileges and Credentialing Web ConferenceApril 3, 200812 – 1 p.m. For audio, call:1-888-850-5066 code 222177#
Association of Washington Public Hospital Districts Sponsored by: Significant funding provided by: Office of Rural Health Policy through the Washington State Department of Health
Speakers Greg Montgomery Dana Livingstone Kenny Robert J. Walerius
Board Responsibility for Medical Staff Privileges and Credentialing Robert J. Walerius
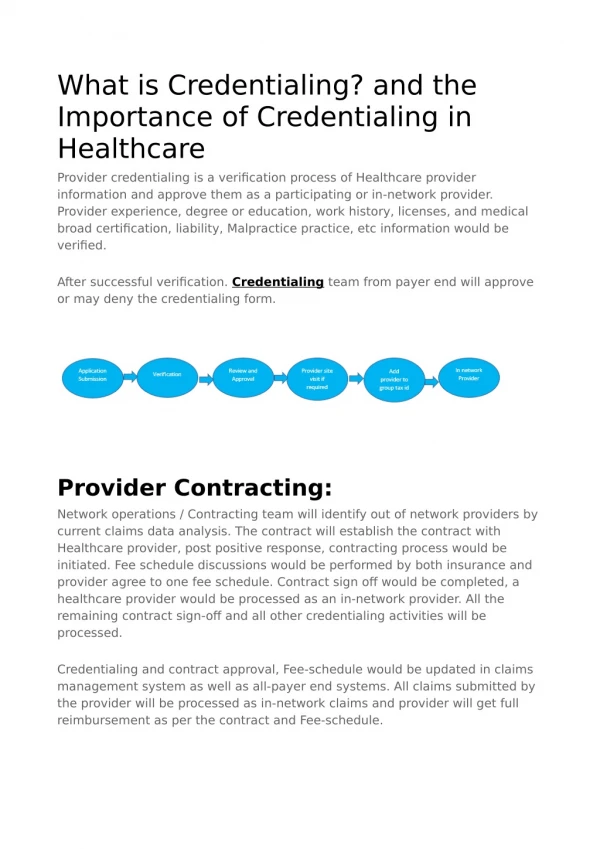
Credentialing = confirming licensure, malpractice insurance, board certification if required, references, restrictions on practice, and background • Privileging = scope of training and current experience to hold clinical privileges requested
Medical Staff Office collects relevant information from applicant and others • File containing application and information is forwarded to the Medical Staff for review and a recommendation to the Board
The Board has ultimate responsibility for approving who can practice in the hospital and what clinical privileges are held • Delegation to the Medical Staff does not relieve the Board of responsibility
A direct correlation exists between the competence of the Medical Staff and quality and patient safety • Quality and safety are core fiduciary responsibilities • We are entering a new area of heightened focus on quality and patient safety
Institute for Healthcare Improvement “5 Million Lives Campaign” • Goal: protect patients from 5 million incidents of harm over 24 months • IHI estimates 15 million incidents of medical harm yearly in hospitals • 40 to 50 incidents of harm for every 100 hospital admissions • 40,000 incidents of harm daily
“5 Million Lives Campaign” (cont’d) • Prior 100,000 Lives Campaign had 3,100 participating hospitals • New campaign seeking 4,000 hospitals • 12 interventions targeted to reduce harm • One intervention is to enlist active governing board support to improve quality
CMS new focus on quality: • “Never Pay” plan – CMS will not reimburse for 8 conditions CMS deems to have occurred because of mistakes – October 1 • Pay for Performance – value-based payment plan • New federal protection rules for confidential reporting of mistakes
Theories of Liability • Board needs to understand theories of liability to evaluate potential risks to the hospital when deciding on privileging
Theories of Liability: (cont’d) • Corporate negligence: • Independent duty to patients to exercise care in selecting, retaining, and supervising the performance of the Medical Staff • Hospital’s role is not just to furnish facilities and equipment for physicians to practice in isolation
Theories of Liability: (cont’d) • Medically unnecessary services: • Patient is unnecessarily exposed to risks of medical procedure and CMS incurs needless costs • CA case – hospital paid $59.5 million to settle false claims allegations that hospital negligently credentialed and monitored cardiologists
Theories of Liability: (cont’d) • Failure of Care: • Care provided is so deficient that it amounts to no care • Liability for billing CMS for services not actually rendered
Board must understand performance goals that will allow the hospital to provide high quality and safe care • Attention to credentialing and privileging is essential to drive increased quality and safety
Suggested Board Questions: • Are the roles of the Board and medical staff clear, understood, and in writing? • Are qualifications for staff membership and privileges in writing and followed?
Board Questions: (cont’d) • What data on clinical competence is reviewed by the medical staff? • Does the medical staff engage in meaningful peer review and corrective action? • Is the Board involved?
Role of the Hospital Board Dana L. Kenny Credentialing / Privileging
Legal Requirements • Accreditation: JCAHO Standards: • 60 WA hospitals JCAHO accredited; 35 not accredited • Governing Board: Sets the framework for supporting quality patient care, treatment and services • Surveys: based upon accreditation cycle (every 36-39 months) • Washington hospital licensing laws (RCW 70.41 and WAC 246-320). Enforcement: • Surveys for compliance every 18 months (except for JCAHO accredited) • Agreement with CMS for Medicare/Medicaid recertification survey
Legal Requirements • CMS Conditions of Participation (42 CFR 482.22) • Hospitals 42 CFR.482.22. Governing Body shall: • Ensure that criteria for selection are individual character, competence, training, experience and judgment • Ensure that the Medical Staff is accountable to the governing body for the quality of care provided to patients • Enforcement: generally delegated to Department of Health by Agreement • Critical Access Hospitals 42 CFR 485.601 • Governing body assumes full legal responsibility for determining, implementing and monitoring policies governing hospital’s total operation.
Legal Requirements • Conditions of Participation: Quality Assessment and Performance Improvement 42 CFR 482 .21. • Governing Body shall: • Ensure that program reflects complexity of hospital and services, involves all hospital departments and focuses on improved health outcomes and the prevention and reduction of medical errors
Meeting Legal RequirementsJCAHO Standards: • Past – general review based upon “paper” credentials • Now – recognition of “active” credentialing • Credentialing/Privileging: collection, verification and assessment of information • More than “paper credentials” required • Objective, evidence-based • Purpose: more comprehensive evaluation of a practitioner’s professional competence
JCAHO Standards: General Competencies 1. Patient Care 2. Medical/Clinical Knowledge 3. Practice-based Learning and Improvement 4. Interpersonal and Communication Skills 5. Professionalism 6. Systems-Based Practice
Privileging: JCAHO Standards • Process for evaluating requests for particular privileges: • Ensuring qualifications based upon ongoing review • For surgeries: developing and approving a procedures list • Assessment of resources • Recommendations to the governing body for applicant-specific privileges
Expedited Credentialing/ Temporary Privileges • Staggered cycles of renewal • Expedited credentialing by Board: when Board not scheduled to meet soon • Cannot be approved by medical staff: • Initial appointment and reappointment • Authority can be delegated to at least two voting members of Board. Otherwise, temporary privileges when: • Complete application awaiting approval (120 days) or • Important patient care need (verification of licensure and current competence) • Process for locums: must meet standards for temporary privileges • Medical staff develops criteria for expedited process for granting privileges
Focused Professional Practice Evaluation Used When: 1. Practitioner has credentials to suggest competence, but additional information needed (initial appointment and anytime additional privileges are granted) 2. Questions arise about practice during course of ongoing practice evaluation
Quality Improvement Programs and Ongoing Professional Practice Evaluation (maintaining privileges) • Quality Improvement Programs: Licensing Requirement. RCW 70.41.200 • Mechanism for periodic review of: • Credentials • Physical and mental capacity • Competence in delivery of health care services • Evaluation of staff privileges
JCAHO Standards • Ongoing professional practice evaluation: • Identifying professional practice trends that impact quality of care and patient safety • Focus on “Continuous Quality Improvement”
Suggested Board Questions: • Does the Medical Staff have: • Process for temporary privileges? Expedited privileges? • Processes for considering “general competencies” for credentialing/privileging? • Process for focused review and ongoing professional practice evaluation?
Peer Review and Corrective Action Greg Montgomery
Peer Review andCorrective Action Scope • Clinical competence refers to judgment regarding the nature and timing of treatment and technical skills in executing the proper treatment • Professional conduct refers to physician conduct when acting in a professional capacity including any impairment or behavior that interferes with the orderly operation of the hospital.
Peer Review and Corrective ActionProfessional Conduct • “Corrective action taken in response to multiple complaints about physician disruptive conduct involving abusive treatment of nurses, technicians, and fellow physicians was appropriate. Clinical incompetence involving patient injury is not a necessary basis for corrective action.” • “The disruptive physician is by definition contentious, threatening, unreachable, insulting and frequently litigious. He will not, or cannot play by the rules, nor is he able to relate to or work well with others.”
Peer Review andCorrective Action Options • Educational • CME • Physician’s assistance programs • Counseling • Proctoring/Preceptoring • Voluntary limitation of privileges • Mandatory second opinion • Suspension • Revocation • Restrictive
Peer Review andCorrective ActionRoad to the Board • Request for corrective action • Investigation and Recommendation to MEC • MEC Recommendation to the Board • Right to Hearing with Report and Recommendation • Right to Appeal
Peer Review andCorrective Action Board’s Role • Hearing Record • Bylaws provide standard
Peer Review andCorrective Action Board’s Role • Appellate Review Committee • Appeal Statement • Oral Presentation • Decision
Peer Review andCorrective Action Immunity • Requirements for immunity for professional review action • Reasonable belief that action was in furtherance of quality health care • Following reasonable effort to obtain facts • After adequate notice and hearing procedures afforded physician • Reasonable belief that action warranted by facts known after reasonable effort to obtain and notice and hearing
Peer Review andCorrective Action Investigation • Physician entitled to a reasonable investigation, not a perfect investigation • “Facts so obviously mistaken or inadequate as to make reliance on them unreasonable” • “Fabricating damaging evidence or purposefully overreacting is not part of legitimate peer review”
Peer Review and Corrective ActionNotice and Hearing • Inform physician of issues • Issues can change during course of investigation as long as there is notice • Opportunity to be heard at each step in process - Investigation Committee, MEC, Fair Hearing, Appeal
Decision • Process • Facts • Conflicts • Conclusions
Peer Review and Corrective Action Key Immunity Question • Was the action undertaken in the reasonable belief that it would further quality health care based on facts known at the time • Courts will not substitute judgment of the medical staff or governing body or reweigh evidence
Robert Walerius –(206) 622-8484 bob.walerius@millernash.com Dana Kenny – (206) 622-8484 dana.kenny@millernash.com Greg Montgomery – (206) 622-8484 greg.montgomery@millernash.com