Download
1 / 13
130 likes | 259 Views
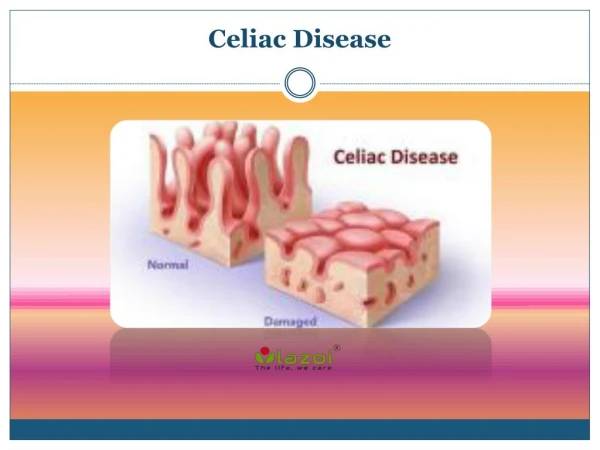
Celiac Disease in Primary Care. Dustin M Adkins Spring 2007. Essentials of Celiac Disease. Autoimmune disorder triggered by gluten “Gluten” is a collective term for the storage proteins of wheat, rye, and barley. Adaptive/innate immune response damages villi in the proximal small intestine

E N D
Celiac Disease in Primary Care Dustin M Adkins Spring 2007
Essentials of Celiac Disease • Autoimmune disorder triggered by gluten • “Gluten” is a collective term for the storage proteins of wheat, rye, and barley. • Adaptive/innate immune response damages villi in the proximal small intestine • Not just GI complaints! A multisystem disorder with highly variable presentation • Increased risk of Non Hodgkins Lymphoma (2.7-6.3x) and overall mortality (1.9-3.4x)
Epidemiology • Not as “rare” as once thought • Affects 1:100 in USA (AGA 2007) • Under-diagnosed
Classical (Textbook) Celiac Disease • Symptoms and complications of malabsorption • Hallmark: Diarrhea/steatorrhea (chronic) • Abdominal distension, edema, extreme lethargy, weight loss, failure to thrive • Onset at any age, gradual or rapid • Often fulfills criteria for IBS. Be suspicious of refractory IBS-D especially with associated celiac symptoms! http://www.pigur.co.il/imgceliac/celiac.jpg
Dermatitis Herpetiformis is “classically” associated with Celiac Disease. Only in a minority of patients. http://webedit.caregroup.org/content/bidmc/Departments/Medicine/Gastroenterology/images/DHimage.jpg http://pathmicro.med.sc.edu/ghaffar/mhcderm.jpg http://merck.micromedex.com/images/bpm/BPM01DE05F09.gif
Atypical Celiac Disease • MOST COMMON presentation • Extra-intestinal manifestations dominate • Blood, Bones, & Babies • Iron deficiency anemia: Unexplained or iron-therapy-refractory (2.3%-5.0%) • Osteoporosis: Premature onset (1.0%-3.4%) • Infertility: Unexplained, recurrent fetal loss (2.1%-4.1%) • Many other S/Sx: short stature, fatigue, delayed puberty, vitamin deficiencies…
Clinical Presentation of Celiac Disease Summary of the clinical presentation of celiac disease. Included 170 biopsy-diagnosed celiac disease patients diagnosed between 1993 and 2000 (Lo 2003).
Asymptomatic Celiac Disease • Often detected when screening 1° relatives, or incidentally during EGD • Risk of complications, lymphoma, mortality still exists!
Autoimmune (10-fold ↑) Thyroiditis (3%) Type I Diabetes (1-12%) Sjögren’s syndrome Addison’s disease Autoimmune liver disease Cardiomyopathy Other related disorders Down syndrome (3-12%) Turners syndrome Williams syndrome Ulcerative colitis Crohns disease IgA nephropathy Occipital calcifications Neuropsychiatric d/o’s Associated Disorders (HLA DQ2/DQ8)
Diagnosis • Anti-tTG IgA is the single most effective test for PCPs! (95% Sens; 98% Spec) • Genetic tests can only rule out Celiac disease (HLA DQ2/DQ8) • Duodenal biopsy (EGD) remains the Gold Standard http://www.glutenfreeworks.com/gluten_explained.php http://www.bidmc.harvard.edu/display.asp?node_id=7715
Difficult task for the patient. Should see a registered dietician Complicated by fast-food lifestyles, hidden ingredients, poor labeling, and costly/unavailable specialty foods. Lifelong diet normalizes mortality/comborbidity risks Treatment: Lifelong Gluten-Free Diet Never advise a patient to start a Gluten-Free Diet before biopsy! It alters the histopathology requiring additional testing ($$$), and ticks off the gastroenterologist!
Lifelong care for the Celiac Patient • Take a good history! Symptom improvement doesn’t mean all gluten has been removed from the diet. • Make sure the patient has support • Celiac support groups • Tons of online info on gluten-free dieting • Work with pharmacist to avoid gluten in drugs • Nardil, Humira, Flonase, Claritin…look it up! • Inactive ingredients (dextri-maltose, dusting powder, starches) • Watch out for anemia, osteoporosis, infertility, and vitamin deficiencies
Participation time! Which is gluten-free? Modified Food Starch Malt Wheat Restaurant Contamination?