Download
1 / 80
1k likes | 3.23k Views
SALIVARY GLANDS. BY PROF. MOHAMED A. EL GHARBAWI e -mail: elgharma2@yahoo.com. OBJECTIVES. Surgical anatomy of different salivary glands Pathology, clinical picture, diagnosis and management of: Salivary Fistula Salivary Stones

E N D
SALIVARY GLANDS BY PROF. MOHAMED A. EL GHARBAWI e-mail: elgharma2@yahoo.com
OBJECTIVES • Surgical anatomy of different salivary glands • Pathology, clinical picture, diagnosis and management of: Salivary Fistula Salivary Stones Inflammation of salivary glands Tumors of salivary glands
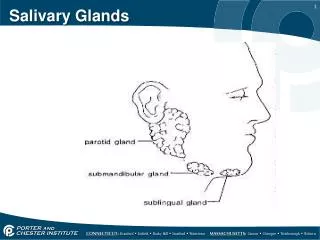
SALIVARY GLANDS • MINOR SALIVARY GLANDS Multiple small scattered in the mouth, lips, tongue and pharynx. • MAJOR SALIVARY GLANDS (PAIRS) 1. PAROTID SALIVARY GLANDS 2. SUBMANDIBULAR SALIVARY GLANDS3. SUBLINGUAL SALIVARY GLANDS
MINOR SALIVARY GLANDS • > 600 minor salivary glands in the oral cavity within its submucosa. • 1-2mm in diameter each • Not encapsulated, only surrounded by connective tissue • Formed of a number of acini connected in a tiny lobule. • May have a common excretory duct with another gland or may have its own excretory duct. • Secretion is mainly mucous and have many functions such as coating the oral cavity with saliva.
PAROTID GLANDS(Must Know) • A pair of glands, 0ne 0n each side • Largest of S Gs • Wedged Behind the mandible between the ramus of the mandible and the mastoid process & upper part of anterior border of Sternocleidomastoid muscle below the external ear
PAROTID GLANDS • Overlies the posterior belly of Digastric muscle and the Styloid process (with 3 muscles attached to it i.e. Stylohyoid, stylopharyngeus and styloglossus m. • Enclosed in a tough sheath called the PARITID FASCIA (from deep cervical fascia) • Septa from the parotid fascia divide the gland into lobules • Upper pole: just below the Zygomatic arch, wedged between the external bony meatus and TM joint
PAROTID GLANDS • 3 structures are entering or leaving theupper pole: 1. Superficial temporal vessels 2. Temporal branches of facial nerve 3. Auriculo temporal nerve • The cervical branch of the facial nerve and the 2 divisions of the posterior facial vein leave the lower pole
PAROTID GLANDS • Anterior border of the gland overlies the masster m. Structures arising from it: 1. The Parotid Duct ( Stenson’s duct): 5cm, runs horizontally across the masseter then pierces the buccinator to open on mm of mouth opposite the 2nd upper molar tooth 2. Zygomatic, Buccal and Mandibular branches of the facial nerve
PAROTID GLANDS • Surface Anatomy : Parotid duct is represented by the middle 1/3 of a line extending from tragus of ear to mid point of a line between ala of nose and angle of mouth • External carotid a. grooves the deep surface of the parotid gland (may pass into its substance) Behind neck of mandible, it divides into 1. Maxillary a. 2. Superficial temporal a.
PAROTID GLANDS • Blood Supply: External Carotid A. & its branches • Venous Drainage: To External Jugular vein • Nerve Supply: Parasympathetic : through the auriculo temporal nerve Sympathetic: from Sympathetic fibers around the external carotid artery
FACIAL NERVE • Emerges through STYLOMASTOID FORAMEN • Main trunk immediately enters the poster- medial aspect of the parotid deeply • Soon it divides into 2 main subdivisions 1. Tempro-facial division 2. Cervico-facial division Facial nerve has 5 terminal branches: Two branches from Tempro-facial division 1.Temporal, 2. Zygomatic, Three branches from Cervico-facial division 3. Buccal 4.Mandibular 5. Cervical
FACIAL NERVE • The 5 branches of the facial nerve pass through the parotid gland at a constant plane superficial to the posterior facial vein • This plane is called the Facio-venous plane (or Plane of Patey) which divide the gland into 2 lobes, Superficial and deep surgical lobes ( Not Anatomical)
SUBMANDIBULAR GLAND • Smaller than Parotid & larger than Sublingual gland • 2 parts * Superficial part: Superficial to Myelhyoid ms. wedged between it and body of mandible ** Deep part: Deep to Myelohyoid ms. Hooking around its posterior border, lying between it and hypoglossus ms. With the lingual n. superior to it and the hypoglossal n. inferiorly
SUBMANDIBULAR GLAND • The Submandibular Duct ( Whartin’s duct) About 5 cm Arises from the anterior end of the deep part Passes anteriorly to open on the side of fraenum lingae Hooked by the lingual nerve, it passes superficial, below and then deep to the duct • Blood Supply: Facial & Lingual artery • Nerve Supply: Submandibular Ganglion
SUBLINGUAL SALIVARY GLAND • Site: lie anterior to the submandibular glandunder the tongue, beneath the mucous membraneof floor of mouth. • Size: it’s the smallest of the 3 S Gs • Shape: almond-shape • Open by many ducts to sublingual fold
SALIVARY FISTULA • TYPES: 1. Internal: Opening into mucosa of buccal cavity, needs no treatment 2. External: Opening into the skin, Saliva is discharged on skin causing eczema, excoriation, inflammation Should be treated
SALIVARY FISTULA • ETIOLOGY: 1. Trauma: Iatrogenic, Stabs 2. Abscess: Spontaneous abscess, I&D 3. Malignant tumors local spread • SALIVARY FISTULA: Connected to the Salivary Gland OR Connected to the Salivary Duct
SALIVARY FISTULA • TREATMENT: A. Fistula Connected to the Salivary Gland: 1. Parotid Gland Fistula Spontaneous Healing is the rule Resistant cases : Use cautary by Diathermy OR Superficial Parotidectomy 2. Submandibular Fistula: Submandibular Sialadenectomy
SALIVARY FISTULA B. Parotid Duct Fistula: 1. Masseteric Fistula: Skin opening lies over the masseter muscle. Difficult to treat. Recent injury is treated by anastomosis of the divided ends over a silk thread. If it fails, Parotiectomy. 2. Premasseteric Fistula: Skin opening lies anterior to border of masseter ms. Easy to treat by splitting the parotid duct in the mouth from the duct orifice to a point proximal to the fistula.
SALIVARY STONES • Etiology: Commoner in Submandibular gland * Submandibular duct ascends ( Independent drain) ** Submandibular secretion is thick *** Food particle may block the opening of the submandibular duct at floor of mouth • Pathology: * Stone in the gland or its duct ** Single or Multiple stones *** Formed of Calcium, Magnesium, Phosphate,Carbonte
SALIVARY STONES • Complications/Fate: * Small stones may migrate unnoticed ** Salivary Colic with migration of bigger stone *** Obstruction & Infection may lead to abscess **** Pressure necrosis may lead to fistula • Symptoms: * Pain (may be colicky) and swelling in submandibular region, increase with meals. ** Irritation of the Lingual nerve (hooking around the duct) may refer pain to tip of tongue /teeth
SALIVARY STONES • Symptoms (Cont.): *** Blood & Pus discharge from the duct opening **** Symptoms of complications if any • Signs: * Give patient lemon to suck, lead to increase pain and swelling ** The gland is enlarged , tender, can’t be rolled around the mandible (LN is rolling)
SALIVARY STONES • Signs (Cont.): *** In floor of mouth, the opening of the duct looks red, raised and discharging blood or pus. Stone may be seen through the opening **** Bimanual Palpation: Gland is better felt through the mouth (LN is better felt outside) • Investigations: * Plain X-ray: Radio-Opaque stone (100%). Rarely radiolucent ** Sialography: Inject radio-opaque dye, Sialactasis
SALIVARY STONES • Treatment: A. Stone in duct: * Meatotomy and Extraction of the stone if it is projecting through the duct opening. ** Splitting of the duct over the stone after fixing it by under running stitch, remove the stone, leave duct wide open for better drainage *** Sialadenectomy for recurrent duct stones B. Stone in the gland: Submandibular Sialadenectomy
Meatotomy , splitting of duct to extract stone & wide drain the duct
INFLAMMATION OF SALIVARY GLANDS • ACUTE A. Acute suppurative sialadenitis & Abscess formation B. Acute viral Parotitis: May be caused by 1. Mumps virus 2. Cytomegalo virus 3. Epstein-Barr virus • CHRONIC 1. Endemic: Parasitic 2. Chronic pyogenic
ACUTE SUPPURATIVE SIALADENITIS Nowadays, bacterial parotitis is rare due to improved standards of living • Predisposing Factors: 1. Bad oral hygeine 2. Debility 3. Dehydration especially post operative 4. Obstruction of the salivary duct by food particles / FB / Stone
ACUTE SUPPURATIVE SIALADENITIS • Organisms: 1. Staphylococcus aureus (Common) 2. Streptococcus (less common) 3. Pneumococci (less common) • Route of entry: 1. From the mouth through the duct 2. Blood born 3. direct spread from a nearby infction
ACUTE SUPPURATIVE SIALADENITIS • Pathology: Parotid > submandibular Gland is congested, swollen and may suppurate • Complications: * Abscess formation ** Extension to near by area (external Auditory meatus, pharynx, neck) *** Salivary fistula if abscess is ruptured **** Submandibular cellulitis (Ludwig’s Angina) ***** Septicemia, Toxemia, Payaemia (pus under pressure) ****** Chronicity and Stone formation
ACUTE SUPPURATIVE SIALADENITIS • CLINICAL PICTURE: Fever, headache, malaise Pain(dull aching then throbbing) Swollen tender edematous gland (Parotid or Sub- mandibular) Opening of gland is red, edematous, may discharge pus Fluctuation is late (Tight parotid fascia)
ACUTE SUPPURATIVE SIALADENITIS • TREATMENT: Prophylaxis: Stop the predisposing factors Conservative treatment: early with no signs of suppuration, Surgery if abscess is suspected with no wait for fluctuation * Physical rest, Analgesic antipyretic **Antibiotics (anti staph. With high concentration in saliva e.g. Clindamycin ***Hot Foments (Local) **** Mouth washes and hygeine ***** No Sialagogues ( Rest to the gland)
ACUTE SUPPURATIVE SIALADENITIS Surgery (Incision & Drainage): *If Conservative treatment fails within 48 hours ** If pus is suspected, Don’t wait for fluctuation (Pain becomes Throbbing, Fever becomes Hectic, Edema becomes Pitting)