Download
1 / 50
630 likes | 1.82k Views
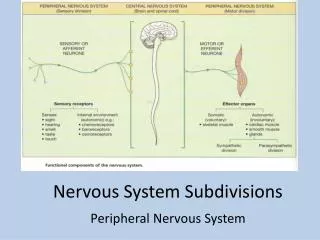
Nervous System Diseases & Disorders. Introduction to Human Diseases Chapter 13. Nervous System Anatomy. Divisions of the nervous system: Central Nervous System Brain and spinal cord Peripheral Nervous System Peripheral nerves Autonomic Nervous System Symphathetic nervous system

E N D
Nervous System Diseases & Disorders Introduction to Human Diseases Chapter 13
Nervous System Anatomy • Divisions of the nervous system: • Central Nervous System • Brain and spinal cord • Peripheral Nervous System • Peripheral nerves • Autonomic Nervous System • Symphathetic nervous system • Parasympathetic nervous system
CNS anatomy • Major parts of the brain • Cerebrum • Cognitive center (thought, memory) • Level of consciousness • Cerebellum • Center of balance & coordination • Brain stem • Center of automatic functions • Blood pressure, respiration, etc.
Meninges • Dura • Outermost layer • Thick, fibrous • Arachnoid • Thin, filmy like a spiderweb • Pia • Thin, vascular layer of loose connective tissue, inseparable from the outer brain surface
Headaches • Any pain occurring in the head • Acute or chronic • Numerous etiologies • Very common condition • May be a symptom of other diseases • Infections, neoplasms, inflammatory diseases, etc.
Headaches • Due to irritation, inflammation of any pain-sensitive structure • Brain itself is not a source of headache • Diagnostic procedures and testing: • Physical exam (PE), CT scan, LP (lumbar puncture or spinal tap), EEG, routine x-rays, MRA, MRI and more
Migraine Headache • Recurrent, usually severe headache of vascular origin • More common in females (3 to 1) • Family history in 70-80% • Onset common in adolescence or early adulthood • 80% have first migraine by 30YOA • Usually become less frequent with age
Migraine Headache • 10-20% US population have migraines • 2nd most common cause of HA in US • Muscle tension HA is #1 • S/S: • Intense throbbing headache, uni-or bilateral • Nausea, vomiting, dizziness, tinnitus • Visual disturbances • With or without aura (classical vs. common) • Duration from 4-72 hours
Migraine Headache • Etiology: • Vasoactive chemicals (peptides) in brain (serotonin and dopamine) • Stimulate inflammatory cascade • This causes vasodilation • Serotonin appears to be most important factor
Subarachnoid Headache • Due to a subarachnoid hemorrhage • 80% SAH due to ruptured intracranial aneurysm • Berry aneurysm, saccular, acquired due to hemodynamic stress at bifurcations • About 28,000 SAH/yr in US • Mean age is 50 YOA • Accounts for 6-8% strokes in US
Subarachnoid Headache • Most common etiology of non-traumatic intracranial hemorrhages • S/S: “worst headache of my life” • Rapid onset, neck stiffness (nuchal rigidity), low back pain, photophobia, nausea & vomiting, seizures in 10-25% • 10% mortality immediately • Up to 60% mortality in 1st month
Head Trauma • #1 cause of trauma deaths in US • Many possible mechanisms of injury: • Falls • Motor vehicle crashes • Assaults
Shaken Baby Syndrome • Vigorous episode of shaking the baby by the arms, torso, or chest • Most victims less than 3 years of age • Produces characteristic injury pattern: • Neurological injury • Mental retardation, seizures, hearing loss • Intracranial hemorrhage or edema, coma • Retinal hemorrhages
Shaken Baby Syndrome • One version of child abuse • First described in 1946 • Part of overall pattern of child abuse: • Multiple fractures • Bruises in all stages of healing, often axial • Often abuse from non-biological parent or caregiver
Shaken Baby Syndrome • Brain injuries: • Hemorrhage (SDH) • Cerebral edema & raised pressure • More common • Prognosis: • 1/3rd mortality • 1/3rd with permanent neurological disabilities
Epidural and Subdural Hematomas • Epidural Hematoma • Hemorrhage above the dura layer • Arterial bleeding • Parietal skull fx, middle meningeal artery • “lucid” interval • Subdural Hematoma • Below the dura • Venous bleeding • More common
EDH & SDH • S/S: • Altered level of consciousness (coma or lethargy), headache • Hemiparesis (right or left) • Unilateral dilated pupil • Treatment: • Neurosurgical drainage of the hematoma
Cerebral Concussion • Disruption of brain function without actual physical brain injury • Typically follows a blow to the head • Often, not always, has loss of consciousness • S/S: headache, nausea, dizziness, amnesias, disorientation, vertigo, photophobia
Concussion • Testing is done to rule out other injuries • Treatment: supportive, observation
Cerebral Contusion • Bruising of the brain tissue • Cerebral edema around the contusion is common • Mechanism: a blow to the head, usually localized force • S/S: headache, variable loss of consciousness, variation from concussion-like symptoms to coma with hemiparesis
Cerebral Contusion • Testing: CT scan to examine extent of brain injury & possible brain herniation • Treatment: variable • Monitoring of ICP, meds to decrease brain swelling, usually surgery is not helpful, other supportive care in ICU
Disorders that cause paralysis • Hemiplegia • Loss of muscle control & sensation on one side of the body (L or R) • Paraplegia • Loss of muscle control & sensation on the lower part of the trunk and lower extremities • Quadriplegia • Paralysis of all four extremities
Hemiplegia • Etiology: most frequently stroke • Also intracranial tumor or hemorrhage • Other S/S: weakness of half of the face, aphasia, agnosia, apraxia, agraphia, alexia, etc.
Paraplegia & Quadriplegia • Etiology: most commonly spinal cord injuries due to trauma • Other S/S: loss of bowel & bladder control, sexual dysfunction • S/S of quadriplegia also include: • Low blood pressure and pulse • Variable loss of respiratory control
CNS Infections • Acute Bacterial Meningitis • Acute inflammation & infection of the CSF & the meninges • Etiology: bacterial, viral, or fungal • Source may be spread from blood or nasopharynx • Most severe type = bacterial • Most common bacteria involved are Strep pneumoniae & Neisseria meningitidis
Acute Bacterial Meningitis • S/S: Headache, nausea, vomiting, fever, seizure, nuchal rigidity, drowsiness, coma • Testing: lumbar puncture makes the diagnosis • Characteristic rash with Neisseria m. • Treatment: antibiotics or antifungals and supportive care
Brain Abscesses • Localized collection of pus • Most commonly in: • Cerebellum • Frontal or temporal lobes of cerebrum • Etiology: spread from some other nearby or distant infection
Brain abscesses • S/S: depending on location, may resemble hemorrhage or CVA • Treatment: • Antibiotics • Surgical drainage of the abscess
Peripheral Nerve Diseases • Peripheral neuritis (peripheral neuropathy) • Noninflammatory degenerative disease of nerve supplying the distal extremities • Commonly males, 30-50 YOA • Etiology: numerous, including alcohol, heavy metal, drug, poisons, TB & infections, diabetes, lupus, nutritional, etc
Peripheral neuropathy • S/S: muscle weakness, paresthesias, pain, tenderness, atrophy, loss of reflexes • Gradual in onset usually • Diagnostics: EMG • Treatment: varies with cause
Bell’s Palsy • Disorder of the facial nerve (cranial nerve VII) • Unilateral paralysis/paresis of the facial muscles • Usually transient • Typically in patients 20-60 YOA
Bell’s Palsy • Etiology: idiopathic technically • Viral etiology is strongly suspected • Autoimmune, ischemic, etc • S/S: facial asymmetry, drooping mouth, drooling, incomplete closure of eye (Bell’s phenomenon) • Treatment: antiviral drugs and steroids usually
Cerebrovascular Accident (CVA) • Focal neurological impairment due to lack of blood supply to an area of the brain lasting more than 24 hours • Clinical condition is called stroke • 2 types of stroke: • Ischemic: embolic or thrombotic, 75% CVA’s • Hemorrhagic: 25% CVA’s
CVA • Risk factors: same as for cardiovascular disease, smoking, HTN, hyperlipidemia, diabetes, etc. TIA’s, oral contraceptives • S/S: hemiplegia or hemiparesis, dysphagia, speech impairment, diplopia & loss of visual fields, lack of coordination, confusion, sensory impairment
CVA • Diagnostics: CT scan to rule out hemorrhage or tumor • Treatment: • Thrombolytic medicines “Clot busters” if stroke symptoms of 3 hrs or less • Supportive care, nutritional, PT & OT
Transient Ischemic Attacks (TIA) • Focal neurological impairment due to transient lack of blood supply to an area of the brain, lasting less than 24 hrs. • TIA’s indicate increased risk of CVA in the future • Resolve completely • Often 20-40 minutes in duration
Transient Ischemic Attacks • Symptoms: most commonly upper extremity clumsiness, weakness, paresthesias, visual field cuts (curtain-like) • Treatment: surgery for carotid plaque, anticoagulants
Epilepsy • Chronic brain disorder characterized by seizures (abnormal, rapid, intense neuronal discharge) • Types of seizures: • Generalized (gran mal) • Involve entire body, unconscious • Partial: part of the body is involve, conscious • Petit mal: momentary, frequent unconscious episodes
Epilepsy • Etiology: mostly idiopathic • Trauma, tumors, CNS infection, drugs & toxins, etc • S/S: in classic generalized seizure • Aura, tonic, clonic, post-ictal phases • Respiratory insufficiency & cyanosis • Incontinence of bowel & bladder
Epilepsy • Treatment: acute and long-term anticonvulsant meds
Degenerative Neurological Diseases • Alzheimer’s Disease • Fatal, long-term disease of the brain • Characterized by neurofibrillary tangles and senile “plaques” • Gradual & permanent deterioration of memory, judgment, cognitive and verbal skills • Geriatric disorder in general
Alzheimer’s Disease • Etiology: unknown • S/S: previous section, end-stage is complete inattention to self • Diagnosis of exclusion • Treatment: some meds slow progression, supportive care of patient and family
Parkinson’s Disease • Movement disorder characterized by muscle rigidity & tremors • Usually males over 65 YOA • Etiology: unknown, related to dopamine deficiency in brain
Parkinson’s Disease • S/S: bradykinesia, involuntary tremors, muscular rigidity • Treatment: dopamine replacement meds, PT, supportive
Multiple Sclerosis (MS) • Chronic, progressive, demyelinating autoimmune disorder • Makes antibodies to myelin • Females (2:1) • Occurs during adult years, not geriatric • About 25,000 new cases/yr in US
MS • S/S: variable, may last hours to weeks • Classically: eye symptoms, paresthesias, paralysis, mood swings, balance problems, often sudden onset with relapses • Treatment: beta-interferon products, corticosteroids, glatiramen acetate (synthetic myelin protein) • Usual cause of death is due to chronic disability issues
Amyotrophic Lateral Sclerosis (ALS) • Adult-onset motor neuron disease • Progressive degeneration & loss of motor function • Called Lou Gehrig’s Disease (1941) • Males between 50-60 YOA • About 6/100,000 adult population in US • 25,000-30,000 cases total in US
ALS • S/S: progressive muscle weakness, atrophy, and fasciculations (twitching) • Eventual involvement of mouth, respiratory muscles, end-stage is complete paralysis • 75-80% begin with limb involvement • Slurred speech, hoarseness, dysphagia, tripping & stumbling, trouble with usual daily activities
ALS • Sporadic form (nonhereditary) 90-95% cases • Inherited version is autosomal dominant • Mean time till ventilator dependent or death: 2-4 years • May survive 5-10 years on ventilator
Cancers of the CNS • Primary brain tumors • Benign or malignant • Most pediatric brain tumors are primary • Examples are astrocytoma, glioblastoma • Secondary brain tumors • Metastases from other sites • Most common tumors of the brain