Download
1 / 20
210 likes | 495 Views
Y-STENTING ASSISTED EMBOLIZATION OF WIDE NECK ANEURYSMS USING FULLY RETRIEVABLE AND DETACHABLE INTRACRANIAL STENT . SOBRI MUDA 1 , RAZALI RALIB 2 , YAZMIN Y 1 , ROZMAN ZAKARIA 1 , AZIZI AB 3 1 Radiology Department, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia.

E N D
Y-STENTING ASSISTED EMBOLIZATION OF WIDE NECK ANEURYSMS USING FULLY RETRIEVABLE AND DETACHABLE INTRACRANIAL STENT SOBRI MUDA1, RAZALI RALIB2, YAZMIN Y1, ROZMAN ZAKARIA1, AZIZI AB3 1Radiology Department, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia. 2Department of Radiology, Kulliyyah (Faculty) of Medicine, International Islamic University Malaysia, Malaysia. 3Department of Neurosurgery, Universiti Kebangsaan Malaysia Medical Centre, Cheras, Kuala Lumpur, Malaysia
INTRODUCTION • Wide necked aneurysms present a challenge to the endovascular therapist • Many techniques had been described to manage these aneurysms • Balloon remodeling • Jailed microcatheter • Horizontal stent assisted • Y-stenting • Stent has few advantages over balloon • Solitaire AB stent is fully retrievable and detachable recently available for intracranial stenting, features not seen in the other type of stents • We present our experience with Y-stenting assisted coiling of wide neck bifurcation aneurysms using Solitaire AB stents
CASE ILLUSTRATION • A 68 years old lady with LOC and GCS of 6/15 • CT scan confirmed SAH and CT angiography showed a wide neck basilar tip aneurysm measuring 5.8 x 6.3 mm, neck measures 4.3 mm • The procedure was performed under GA and patient already on a long term dual antiplatelet (clopidogrel and aspirin) for ischemic heart disease • Bilateral common femoral artery punctures were done. A 6F guiding catheter with continuous heparinized flushing system
A microcatheter (Prowler 0.021”, Cordis) with GT double curve microwire (Terumo) was advanced into the left P1 segment • A fully retrievable and detachable stent (Solitaire AB, ev3; 4mm x 20mm) was delivered and fully deployed but not detached • Then a second stent was navigated into right P1 segment through 1st stent mesh and deployed and detached to form a Y configuration • Loose coiling of the basilar tip aneurysm was performed using 2 detachable coils • She was discharged after 3 weeks in intensive care unit (ICU) and 2 weeks in general ward, ambulating with assistance.
CASE ILLUSTRATION A 54 yo presented with frequent headache. CT brain followed by CT angiogram revealed a large wide neck left MCA aneurysm measuring 11.1 x 11.2 mm with the neck measuring 5.2mm and a small lobulated Pcom. No evidence of rupture He’d embolization of the left Pcom aneurysm initially. We did a Y-stenting assisted embolization of the large left MCA aneurysm in a different session Clopidogrel 75mg daily and aspirin 150mg daily were started 5 days prior to the procedure. EVT was done under general anaesthesia. Bilateral common femoral artery punctures with 6F guiding catheters were used We decided to use the Solitaire AB stent (ev3) combined with LEO stent (Balt) to form a Y-configuration and loosely coil the aneurysm
A microcatheter (Prowler 0.021”, Cordis) used. The Solitaire AB stent (ev3) was then delivered and fully deployed but not detached • The microcatheter (Prowler 0.021”, Cordis) was then pushed through the stent struts. A Leo stent (Balt; 2.5mm x 18mm) was delivered • After both stents formed a proper Y configuration with patency of both MCA branches. The stent then detached. • The aneurysm was then loosely packed • Patient was well post procedure and discharged 4 days later.
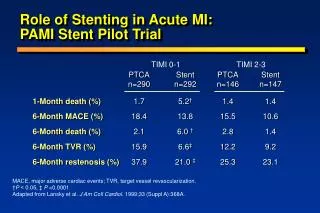
DISCUSSION • Stents had revolutionized the treatment of wide neck aneurysms; • Provided structural support for coil embolization • Preventing coil herniation • Allowing increased packing density • Impact on flow diversion • Wide neck aneurysms arising from vessel bifurcation provides a bigger challenge • Two methods had been described are horizontal and Y-stenting
DISCUSSION • Lozen et al described 6 patients with Y configuration using Neuroform stents (Boston Scientific Neurovascular) but in 1 patient – friction. Lozen A et al. (2009) Y-stent-assisted coil embolization for the management of unruptured cerebral aneurysms: report of six cases. Acta neurochirurgica 151:1663-1672 • We believe by having the capability to still ‘hold’ the stent via it’s delivery wire, the friction can be better manage • And we’ve the option to fully retrieve back the stent • Rohde et al described a Y-stenting Acom aneurysm with Enterprise stents. Rohde S et al. (2009) Treatment of a wide-necked aneurysm of the anterior cerebral artery using two Enterprise stents in "Y"-configuration stenting technique and coil embolization: a technical note. Neuroradiology • Close cell design stent, there was difficulty to push in the microcatheter through the stent struts • With the control and ‘holding’ features, we can reduce the risk of stent displacement
DISCUSSION • In both of our patients, we did not have any difficulties in navigating the microcatheter through the Solitaire AB stent strut and also deploying the second stent through the first stent struts • In the second patient with middle cerebral artery bifurcation aneurysm, the Leo stent (Bard) was used as the second stent for the Y configuration, with similar ease.
CONCLUSION • Treatment of wide necked bifurcation aneurysm with Y-stenting technique is safe and effective • Usage of fully retrievable and detachable stent in Y-stenting; • Reduce risk of stent displacement • Good control of 1st stent during microcatheter crossing for 2nd stent • Allows repositioning of a fully deployed stent • Able to combine with other type of stent