Download
1 / 50
901 likes | 2.21k Views
Cerebrovascular Disease. Section 1 General consideration. Cerebrovascular disease: any abnormality of the brain resulting from a pathologic process of the blood vessels.

E N D
Section 1 General consideration • Cerebrovascular disease: any abnormality of the brain resulting from a pathologic process of the blood vessels. • Cerebrovascular accident orstroke may be defined as a sudden interruption of blood supply or hemorrhage into apart of the brain. • the third commonest cause of death
Classification • Ischemic transient ischemic attack (TIA) cerebral thrombosis cerebral embolism cerebral infarction lacunar infarct • Hemorrhagic cerebral hemorrhage subarachnoid hemorrhage (SAH)
Blood supply of brain • 1. Internal carotid system Branchiocephalic trunk→right common carotid artery left common carotid artery →internal carotid artery → carotid foramen → • Ophthalmic artery • Anterior choroidal artery • Posterior communicating artery • Anterior cerebral artery • Middle cerebral artery
Supply eyes and anterior 3/5 of the brain: frontal, parietal, part of temporal lobe, basal ganglia.
Blood supply of brain • 2. Vertebral-basilar system • Subclavian artery → vertebral artery → C6-C1 transverse foramen → great occipital foramen → basilar artery • posterior spinal arteries, anterior spinal artery • posterior inferior cerebellar artery • auditory artery • posterior cerebral arteries
supply cerebellum, brain stem, posterior 2/5 of brain (occipital, part of tempral lobe)
Blood supply of brain • 3. Circle of Willis
Blood supply of brain • This forms a unique anastomotic system at the base of the brain between the internal carotid and vertebral-basilar systems. internal carotid arteries two anterior cerebral arteriesanterior communicating artery two posterior cerebral arteries two posterior communicating arteries
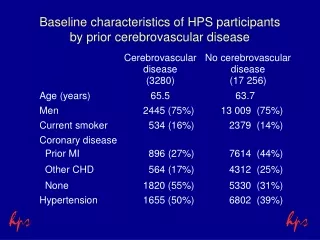
Risk factors of CVD • Age, family history, race • Hypertension • Heart disease • Diabetes • Hyperlipemia • Smoking, excessive drinking • Obesity, diet, contraceptive drugs
Section 2 TIA • A transient ischemic attack is a focal disturbance of the cerebral circulation, frequently repetitive, resulting in a period of impaired function lasting for a short period (anything from a few minutes to twenty-four hours). Attacks can occur in the carotid and/or vertebral artery territories.
Etiology • Micro embolism • Spasm of cerebral blood vessel • Hemodynamic change • Compression of vertebral artery, steal syndrome
Clinical feature 1. 50-70, M>F characteristics: • Abrupt onset • Transient • Complete recovery • Repetitive
Clinical feature 2. Transient carotid ischemic attacks (1)Common symptoms: • Weakness of the contralateral arm and/or leg. (2) Characteristic symptoms: • Transient loss of vision in the eye contralateral to the paresis (amaurosis fugax). • Horner sign (3) Symptoms may present: • Dysphasia • Paraesthesia or numbness in the contralateral limbs. • hemianopia
Clinical feature 3. Transient vertebral –basilar ischemic attack (1) Common symptoms • Vertigo, nausea, vomiting (2) Characteristic symptoms: • Drop attack • Transient global amnesia, TGA • Cortical blindness • Crossed paralysis or sensory disturbance
Clinical feature (3) Symptoms may present: • Dysphagia, dysarthria • Ataxia • Disturbance of consciousness • diplopia
Diagnosis • clinical features • No signs between attack
Differential diagnosis • Partial epilepsy • Meniere disease
Treatment 1. Etiologic therapy • Blood pressure, sugar, lipid • Carotid endarterectomy, anastomosis of extra-intra cranial vessels 2. Prophylactic treatment • Anti-platelet aggregation drugs: Aspirin 50-300mg Qd Po Ticlopidine 250mg Qd Po
Treatment 2. Prophylactic treatment • Anticoagulants: heparin • Chinese herbs Chuanxiong rhizome, Red sage root, Saf flower • Others: vessodilator, volume expensor (Dextran-40) 3. Brain protective agents • Calcium antagonist: nimodipine 20-40mg tid po flunarizine (Sibelium) 5mg Qn po
Prognosis • 1/3 → repetitive attack • 1/3 → remission • 1/3 → cerebral infarction
Section 3 Cerebral Thrombosis • infarction of an area of the brain secondary to arterial occlusion by thrombosis of a major vessel with insufficient collateral circulation.
Etiology • atherosclerosis • Arteritis: such as leptospirosis, rheumatic fever • rare cause: congenital vascular malformation, polycythemia blood hypercoagulability
Pathology • Vessel: carotid > middle > posterior > anterior > vertebral-basilar • Super-early stage: 1-6 hour • Necrosis→ cyst • White infarct • Red infarct: hemorrhagic infarct
Pathophysiology • Neurons are sensitive to ischemia • Central necrosis • Ischemic penumbra • Super early stage: < 6 hours
Clinical feature • onset is rapid • usually occur in the rest and sleep • premonitory symptoms such as weakness of a limb, transient ischemic attack • The headache, vomit, and loss of consciousness may be absent or slight. • Focal signs develop in several days
Clinical type • Complete stroke • Progressive stroke • Reversible ischemic neurological deficit, RIND)
Clinical syndrome 1. Internal carotid artery • May have no signs (if the collateral supply, from the other side, is good ) • amaurosis fugax, uniocular blindness • Horner's syndrome may present in the side of the occlusion. • contralateral hemiplegia and hemianesthesia.
Clinical syndrome 2. Middle cerebral artery • contralateral hemiplegia, hemianesthesia, hemianopia • aphasia (if the dominant hemisphere is affected) • Disturbance of body image (non-dominant hemisphere)
Clinical syndrome 3. Anterior cerebral artery • contralateral hemiplegia, the leg frequently being more affected than the arm. • paracentral lobule: regulation of sphincter function, retention or incontinence • mental symptoms: apathy, euphoria
Clinical syndrome 4. Posterior cerebral artery • contralateral hemianopia or quadrantanopia • thalamic syndrome: contralateral hemianesthesia, thalamic pain, ataxia, tremor, athetosis
Clinical syndrome 5. Vertebro-basilar artery (1) Main trunk • nausea, vomiting,tetraplegia, coma, death (2) Weber syndrome • Unilateral lesion of midbrain • Ipsilateral oculomotor nerve paralysis, contra lateral hemiplegia
Clinical syndrome • (3) locked-in syndrome • Bilateral infarction in the basis pontis • Tetraplegia, can not speak, can not swallow • Conscious • Can only respond by vertical gaze and blinking
Clinical syndrome 6. posterior inferior cerebellar artery Wallenberg's syndrome, Lateral medullary syndrome • Vertigo, vomiting, nystagmus • Crossed sensory disturbance • Ipsilateral Horner sign • Dysphagia, dysarthria • Ipsilateral ataxia
Investigation 1. CT Low density focus after 24-48 hours
Investigation A right carotid artery occlusion, low signal of T1, and high signal of T2 weighted image. • 2. MRI
Investigation 3. Lumbar puncture • Normal. • Large infarct: pressure ↑ • Hemorrhagic infarction: RBC 4. DSA 5. TCD
Diagnosis • after middle or old age. • rapid onset focal cerebral symptoms • premonitory symptoms • occurs in rest or sleep • CT/MRI find cerebral infarction focus
Differential diagnosis • Cerebral hemorrhage • Cerebral embolism • Intracranial tumor
Treatment 1. Principle 2. Fibrinolytic therapy of super-early stage • Within 6 hours • Urokinase, rt-PA 3. Anticoagulant • Heparin, low molecular heparin 4. Brain protect • Calcium antagonist: nimodipine, flunarizine • Mannitol • Hypothermia
Treatment 5. Fibrinogen degradation • Defibrase, Batroxobin 6. Anti platelet aggregation • Aspirin, Ticlopidine 7. Others • ? Vessel dilator • ? Metabolic activator
Treatment 8. Surgical treatment • Reduce intracranial pressure 9. General management • Reduce intracranial pressure: mannitol 10. Stroke unit 11. Rehabilitation 12. Prophylactic treatment • Aspirin, Ticlopidine
Pathology • 3-4mm, <15-20mm • Small liquid cavity • Basal ganglia, thalamus, brain stem • Small artery: 100-200μm • Atherosclerosis
Clinical feature • 40-60 years of age • Always combined with hypertension Lacunar syndrome: • 1. Pure motor hemiparesis • 2. Pure sensory stroke • 3. Ataxic-hemiparesis • 4. Dysarthric-clumsy hand syndrome • 5. Sensorimotor stroke • 6. Lacunar state
Cerebral embolism Occlusion of a major cerebral artery by an embolus, with resultant infarction of part of the brain.
Etiology • Cardiac cause: Atrial fibrillation, rheumatic valve disease, endocarditis, atrial myxoma, myocardial infarction • Non-cardiac: Atherosclerosis plaque, pus embolus, fat embolus, tumor embolus • Embolus of unknown origin
Clinical feature • Left middle cerebral artery • abrupt onset, maximum disability occurring at once • In some cases, there is rapid improvement • The primary disease, such as rheumatic heart disease
Treatment • Cerebrovasodilators • Anticoagulant therapy • Treatment of primary disease